
Page 127 - Manual of Equine Field Surgery
P. 127
lntraoral Wire Fixation of Rostral Mandibular and Maxillary Fractures 123
debridement of the fracture site. Remaining food to facilitate wire passage between the incisors. The
material, clotted blood, and bone fragments are wires should be applied tightly by hand and
removed. A bone curette may be used to freshen twisted one or two turns followed by additional
the edges of exposed bone, being careful to not twisting using fencing pliers, needle drivers, or the
manipulate or damage exposed, unerupted per- equivalent, being careful not to overtighten the
rnanent teeth. Completely detached or broken wires and cause wire breakage. When necessary,
teeth should be removed. However, loose decidu- additional stabilization can be achieved by secur-
ous teeth are maintained if possible. These teeth ing the corner incisor(s) to the exposed canine
often survive better than expected and provide if erupted or second or third premolar (Figures
stability, structure, and positioning for future 20-2 and 20-4).
permanent tooth eruption. Fractures involving Incorporating the second premolar into the
alveoli can result in infectious periodontitis and fixation involves placing a tension band wire from
the incisors to the second premolar (Figure 20-3).
pulpitis, necessitating removal of the tooth.9
However, removal of the tooth should be delayed A stab incision is made through the cheek directly
until the fracture heals. over the space between the second and third
Fractures that involve four or fewer incisors premolars. Hemorrhage is minimized by incising
can be repaired with cerclage wire fixation tech- through the skin and using blunt dissection to
niques. As a rule of thumb, wires should engage a separate underlying soft tissues. T11e buccal
minimum of two teeth as the teeth immediately mucosa is penetrated, and the drill bit with a pro-
adjacent to the fracture will not be very stable. A tective drill guide is positioned between the
minimum of two loops should be used to secure second and third premolars just ventral to the gin-
a fracture fragment. Ideally, there should be gival margin. The drill guide is left in place after
overlap of the wire loops to improve stabilization drilling between the teeth is completed to help
(Figure 20-1). A 14-gauge hypodermic needle thread the wire through the drilled hole. The wire
with or without a 2-mm drill hole can be used to is then pulled through the cheek and directed
guide the stainless steel wire ( 16 to 18 gauge [ 1- rostral to be laced through the holes previously
to 1.2-mm diameter]) through the interalveolar made between the incisors. The wires spanning the
spaces. In young horses, the 14-guage needle may interdental space are twisted together to increase
be used without prior drilling. The 14-guage compression at the fracture line. After tightening,
needle may also be used as a cannula after drilling the ends of the wires are bent fl.at and may be
I
'
I .
A B c
7iit?~r ,v- (:.,,,_..
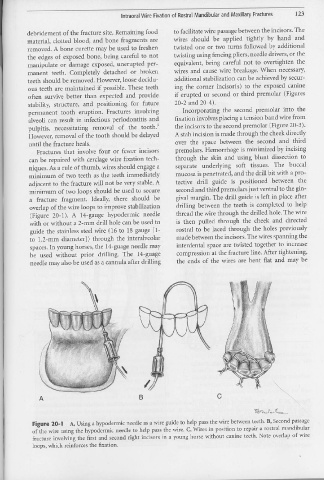
Figure 20-1 A, Using a hypodermic needle as a wire guide to help pass the wire between teeth. B, Second passage
of the wire using the hypodermic needle to help pass the wire. C, Wires in position to repair a rostral mandibular
fracture involving the first and second right incisors in a young horse without canine teeth. Note overlap of wire
loops, which reinforces the fixation.