
Page 28 - Prestige Brochures & Enrollment Packet
P. 28
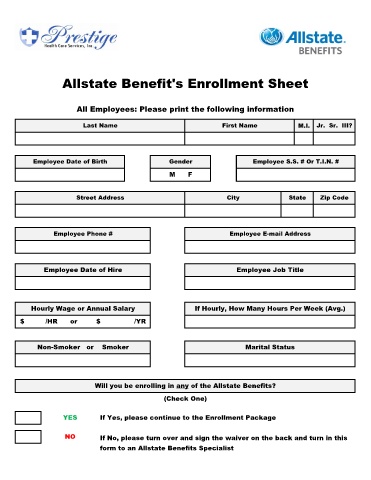
Allstate Benefit's Enrollment Sheet
All Employees: Please print the following information
Last Name First Name M.I. Jr. Sr. III?
Employee Date of Birth Gender Employee S.S. # Or T.I.N. #
M F
Street Address City State Zip Code
Employee Phone # Employee E-mail Address
Employee Date of Hire Employee Job Title
Hourly Wage or Annual Salary If Hourly, How Many Hours Per Week (Avg.)
$ /HR or $ /YR
Non-Smoker or Smoker Marital Status
Will you be enrolling in any of the Allstate Benefits?
(Check One)
YES If Yes, please continue to the Enrollment Package
NO If No, please turn over and sign the waiver on the back and turn in this
form to an Allstate Benefits Specialist