
Page 52 - 2023 All Products
P. 52
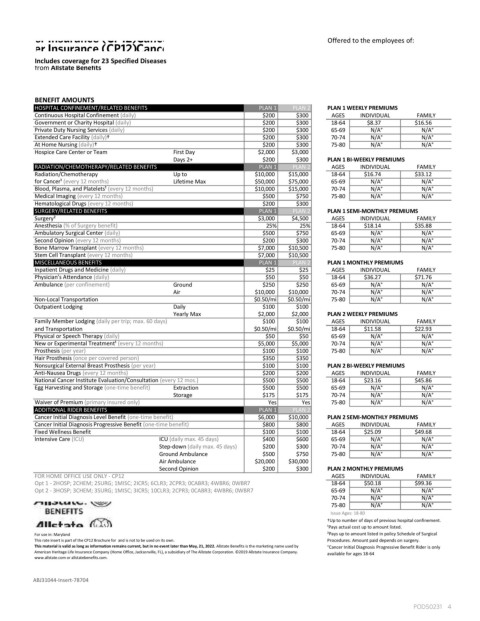
Offered to the employees of:
Includes coverage for 23 Specified Diseases
from Allstate Benefits
BENEFIT AMOUNTS
HOSPITAL CONFINEMENT/RELATED BENEFITS PLAN 1 PLAN 2 PLAN 1 WEEKLY PREMIUMS
Continuous Hospital Confinement (daily) $200 $300 AGES INDIVIDUAL FAMILY
Government or Charity Hospital (daily) $200 $300 1864 $8.37 $16.56
Private Duty Nursing Services (daily) $200 $300 6569 N/A° N/A°
Extended Care Facility (daily)† $200 $300 7074 N/A° N/A°
At Home Nursing (daily)† $200 $300 7580 N/A° N/A°
Hospice Care Center or Team First Day $2,000 $3,000
Days 2+ $200 $300 PLAN 1 BIWEEKLY PREMIUMS
RADIATION/CHEMOTHERAPY/RELATED BENEFITS PLAN 1 PLAN 2 AGES INDIVIDUAL FAMILY
Radiation/Chemotherapy Up to $10,000 $15,000 1864 $16.74 $33.12
for Cancer¹ (every 12 months) Lifetime Max $50,000 $75,000 6569 N/A° N/A°
Blood, Plasma, and Platelets¹ (every 12 months) $10,000 $15,000 7074 N/A° N/A°
Medical Imaging (every 12 months) $500 $750 7580 N/A° N/A°
Hematological Drugs (every 12 months) $200 $300
SURGERY/RELATED BENEFITS PLAN 1 PLAN 2 PLAN 1 SEMIMONTHLY PREMIUMS
Surgery² $3,000 $4,500 AGES INDIVIDUAL FAMILY
Anesthesia (% of Surgery benefit) 25% 25% 1864 $18.14 $35.88
Ambulatory Surgical Center (daily) $500 $750 6569 N/A° N/A°
Second Opinion (every 12 months) $200 $300 7074 N/A° N/A°
Bone Marrow Transplant (every 12 months) $7,000 $10,500 7580 N/A° N/A°
Stem Cell Transplant (every 12 months) $7,000 $10,500
MISCELLANEOUS BENEFITS PLAN 1 PLAN 2 PLAN 1 MONTHLY PREMIUMS
Inpatient Drugs and Medicine (daily) $25 $25 AGES INDIVIDUAL FAMILY
Physician’s Attendance (daily) $50 $50 1864 $36.27 $71.76
Ambulance (per confinement) Ground $250 $250 6569 N/A° N/A°
Air $10,000 $10,000 7074 N/A° N/A°
NonLocal Transportation $0.50/mi $0.50/mi 7580 N/A° N/A°
Outpatient Lodging Daily $100 $100
Yearly Max $2,000 $2,000 PLAN 2 WEEKLY PREMIUMS
Family Member Lodging (daily per trip; max. 60 days) $100 $100 AGES INDIVIDUAL FAMILY
and Transportation $0.50/mi $0.50/mi 1864 $11.58 $22.93
Physical or Speech Therapy (daily) $50 $50 6569 N/A° N/A°
New or Experimental Treatment¹ (every 12 months) $5,000 $5,000 7074 N/A° N/A°
Prosthesis (per year) $100 $100 7580 N/A° N/A°
Hair Prosthesis (once per covered person) $350 $350
Nonsurgical External Breast Prosthesis (per year) $100 $100 PLAN 2 BIWEEKLY PREMIUMS
AntiNausea Drugs (every 12 months) $200 $200 AGES INDIVIDUAL FAMILY
National Cancer Institute Evaluation/Consultation (every 12 mos.) $500 $500 1864 $23.16 $45.86
Egg Harvesting and Storage (onetime benefit) Extraction $500 $500 6569 N/A° N/A°
Storage $175 $175 7074 N/A° N/A°
Waiver of Premium (primary insured only) Yes Yes 7580 N/A° N/A°
ADDITIONAL RIDER BENEFITS PLAN 1 PLAN 2
Cancer Initial Diagnosis Level Benefit (onetime benefit) $6,000 $10,000 PLAN 2 SEMIMONTHLY PREMIUMS
Cancer Initial Diagnosis Progressive Benefit (onetime benefit) $800 $800 AGES INDIVIDUAL FAMILY
Fixed Wellness Benefit $100 $100 1864 $25.09 $49.68
Intensive Care (ICU) ICU (daily max. 45 days) $400 $600 6569 N/A° N/A°
Stepdown (daily max. 45 days) $200 $300 7074 N/A° N/A°
Ground Ambulance $500 $750 7580 N/A° N/A°
Air Ambulance $20,000 $30,000
Second Opinion $200 $300 PLAN 2 MONTHLY PREMIUMS
FOR HOME OFFICE USE ONLY CP12 AGES INDIVIDUAL FAMILY
Opt 1 2HOSP; 2CHEM; 2SURG; 1MISC; 2ICR5; 6CLR3; 2CPR3; 0CABR3; 4WBR6; 0WBR7 1864 $50.18 $99.36
Opt 2 3HOSP; 3CHEM; 3SURG; 1MISC; 3ICR5; 10CLR3; 2CPR3; 0CABR3; 4WBR6; 0WBR7 6569 N/A° N/A°
7074 N/A° N/A°
7580 N/A° N/A°
Issue Ages: 1880
†Up to number of days of previous hospital confinement.
¹Pays actual cost up to amount listed.
For use in: Maryland ²Pays up to amount listed in policy Schedule of Surgical
This rate insert is part of the CP12 Brochure for and is not to be used on its own. Procedures. Amount paid depends on surgery.
This material is valid as long as information remains current, but in no event later than May, 21, 2022. Allstate Benefits is the marketing name used by °Cancer Initial Diagnosis Progressive Benefit Rider is only
American Heritage Life Insurance Company (Home Office, Jacksonville, FL), a subsidiary of The Allstate Corporation. ©2019 Allstate Insurance Company. available for ages 1864
www.allstate.com or allstatebenefits.com.
ABJ31044Insert78704
�������� �