
Page 31 - NCISS Your Advocate April 2020
P. 31
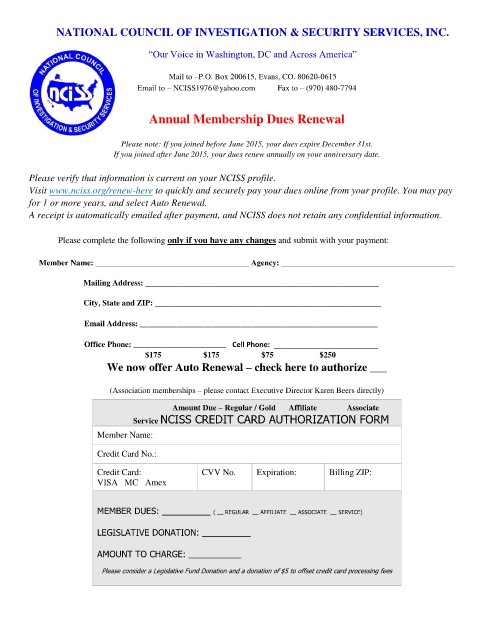
NATIONAL COUNCIL OF INVESTIGATION & SECURITY SERVICES, INC.
“Our Voice in Washington, DC and Across America”
Mail to –P.O. Box 200615, Evans, CO. 80620-0615
Email to – NCISS1976@yahoo.com Fax to – (970) 480-7794
Annual Membership Dues Renewal
Please note: If you joined before June 2015, your dues expire December 31st.
If you joined after June 2015, your dues renew annually on your anniversary date.
Please verify that information is current on your NCISS profile.
Visit www.nciss.org/renew-here to quickly and securely pay your dues online from your profile. You may pay
for 1 or more years, and select Auto Renewal.
A receipt is automatically emailed after payment, and NCISS does not retain any confidential information.
Please complete the following only if you have any changes and submit with your payment:
Member Name: ______________________________________ Agency: ___________________________________________
Mailing Address: __________________________________________________________
City, State and ZIP: ________________________________________________________
Email Address: ___________________________________________________________
Office Phone: _______________________ Cell Phone: __________________________
$175 $175 $75 $250
We now offer Auto Renewal – check here to authorize ___
(Association memberships – please contact Executive Director Karen Beers directly)
Amount Due – Regular / Gold Affiliate Associate
Service NCISS CREDIT CARD AUTHORIZATION FORM
Member Name:
Credit Card No.:
Credit Card: CVV No. Expiration: Billing ZIP:
VISA MC Amex
MEMBER DUES: __________ ( __ REGULAR __ AFFILIATE __ ASSOCIATE __ SERVICE)
LEGISLATIVE DONATION: __________
AMOUNT TO CHARGE: _______________
Please consider a Legislative Fund Donation and a donation of $5 to offset credit card processing fees