
Page 192 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 192
178 SECTION III Cardiovascular-Renal Drugs
Vasodilator
drugs
Decreased
systemic
vascular
resistance
Decreased 1 Decreased Increased
renal arterial sympathetic
sodium pressure nervous system
excretion outflow
2
Increased
renin
1 release
2 2
Increased Increased Increased Decreased
Increased Increased systemic heart cardiac venous
aldosterone angiotensin II vascular rate contractility capacitance
resistance
Sodium retention, Increased Increased
increased plasma arterial cardiac
volume pressure output
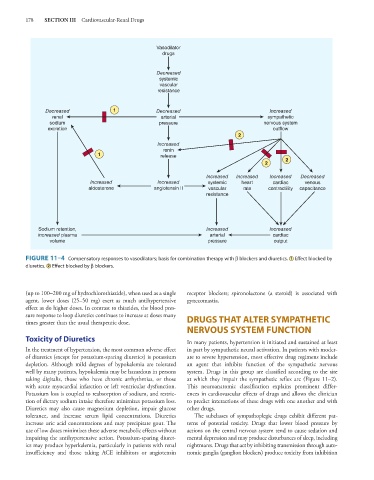
FIGURE 11–4 Compensatory responses to vasodilators; basis for combination therapy with β blockers and diuretics. 1 Effect blocked by
diuretics. 2 Effect blocked by β blockers.
(up to 100–200 mg of hydrochlorothiazide), when used as a single receptor blockers; spironolactone (a steroid) is associated with
agent, lower doses (25–50 mg) exert as much antihypertensive gynecomastia.
effect as do higher doses. In contrast to thiazides, the blood pres-
sure response to loop diuretics continues to increase at doses many
times greater than the usual therapeutic dose. DRUGS THAT ALTER SYMPATHETIC
NERVOUS SYSTEM FUNCTION
Toxicity of Diuretics In many patients, hypertension is initiated and sustained at least
In the treatment of hypertension, the most common adverse effect in part by sympathetic neural activation. In patients with moder-
of diuretics (except for potassium-sparing diuretics) is potassium ate to severe hypertension, most effective drug regimens include
depletion. Although mild degrees of hypokalemia are tolerated an agent that inhibits function of the sympathetic nervous
well by many patients, hypokalemia may be hazardous in persons system. Drugs in this group are classified according to the site
taking digitalis, those who have chronic arrhythmias, or those at which they impair the sympathetic reflex arc (Figure 11–2).
with acute myocardial infarction or left ventricular dysfunction. This neuroanatomic classification explains prominent differ-
Potassium loss is coupled to reabsorption of sodium, and restric- ences in cardiovascular effects of drugs and allows the clinician
tion of dietary sodium intake therefore minimizes potassium loss. to predict interactions of these drugs with one another and with
Diuretics may also cause magnesium depletion, impair glucose other drugs.
tolerance, and increase serum lipid concentrations. Diuretics The subclasses of sympathoplegic drugs exhibit different pat-
increase uric acid concentrations and may precipitate gout. The terns of potential toxicity. Drugs that lower blood pressure by
use of low doses minimizes these adverse metabolic effects without actions on the central nervous system tend to cause sedation and
impairing the antihypertensive action. Potassium-sparing diuret- mental depression and may produce disturbances of sleep, including
ics may produce hyperkalemia, particularly in patients with renal nightmares. Drugs that act by inhibiting transmission through auto-
insufficiency and those taking ACE inhibitors or angiotensin nomic ganglia (ganglion blockers) produce toxicity from inhibition