
Page 689 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 689
CHAPTER 37 Hypothalamic & Pituitary Hormones 675
Oocyte
retrieval & Embryo
fertilization transfer
hCG
Gonadotropin
Progesterone
Time (days) Menses
GnRH agonist
or
GnRH
antagonist
Luteal phase Follicular phase Luteal phase
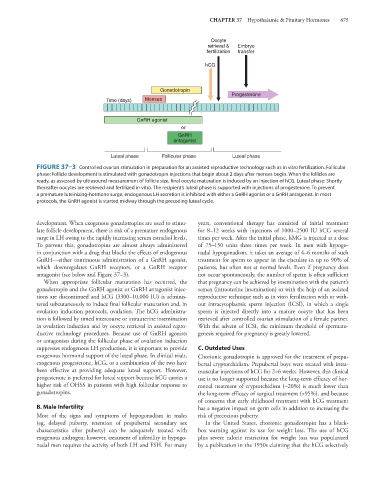
FIGURE 37–3 Controlled ovarian stimulation in preparation for an assisted reproductive technology such as in vitro fertilization. Follicular
phase: Follicle development is stimulated with gonadotropin injections that begin about 2 days after menses begin. When the follicles are
ready, as assessed by ultrasound measurement of follicle size, final oocyte maturation is induced by an injection of hCG. Luteal phase: Shortly
thereafter oocytes are retrieved and fertilized in vitro. The recipient’s luteal phase is supported with injections of progesterone. To prevent
a premature luteinizing-hormone surge, endogenous LH secretion is inhibited with either a GnRH agonist or a GnRH antagonist. In most
protocols, the GnRH agonist is started midway through the preceding luteal cycle.
development. When exogenous gonadotropins are used to stimu- years, conventional therapy has consisted of initial treatment
late follicle development, there is risk of a premature endogenous for 8–12 weeks with injections of 1000–2500 IU hCG several
surge in LH owing to the rapidly increasing serum estradiol levels. times per week. After the initial phase, hMG is injected at a dose
To prevent this, gonadotropins are almost always administered of 75–150 units three times per week. In men with hypogo-
in conjunction with a drug that blocks the effects of endogenous nadal hypogonadism, it takes an average of 4–6 months of such
GnRH—either continuous administration of a GnRH agonist, treatment for sperm to appear in the ejaculate in up to 90% of
which downregulates GnRH receptors, or a GnRH receptor patients, but often not at normal levels. Even if pregnancy does
antagonist (see below and Figure 37–3). not occur spontaneously, the number of sperm is often sufficient
When appropriate follicular maturation has occurred, the that pregnancy can be achieved by insemination with the patient’s
gonadotropin and the GnRH agonist or GnRH antagonist injec- semen (intrauterine insemination) or with the help of an assisted
tions are discontinued and hCG (3300–10,000 IU) is adminis- reproductive technique such as in vitro fertilization with or with-
tered subcutaneously to induce final follicular maturation and, in out intracytoplasmic sperm injection (ICSI), in which a single
ovulation induction protocols, ovulation. The hCG administra- sperm is injected directly into a mature oocyte that has been
tion is followed by timed intercourse or intrauterine insemination retrieved after controlled ovarian stimulation of a female partner.
in ovulation induction and by oocyte retrieval in assisted repro- With the advent of ICSI, the minimum threshold of spermato-
ductive technology procedures. Because use of GnRH agonists genesis required for pregnancy is greatly lowered.
or antagonists during the follicular phase of ovulation induction
suppresses endogenous LH production, it is important to provide C. Outdated Uses
exogenous hormonal support of the luteal phase. In clinical trials, Chorionic gonadotropin is approved for the treatment of prepu-
exogenous progesterone, hCG, or a combination of the two have bertal cryptorchidism. Prepubertal boys were treated with intra-
been effective at providing adequate luteal support. However, muscular injections of hCG for 2–6 weeks. However, this clinical
progesterone is preferred for luteal support because hCG carries a use is no longer supported because the long-term efficacy of hor-
higher risk of OHSS in patients with high follicular response to monal treatment of cryptorchidism (~20%) is much lower than
gonadotropins. the long-term efficacy of surgical treatment (>95%), and because
of concerns that early childhood treatment with hCG treatment
B. Male Infertility has a negative impact on germ cells in addition to increasing the
Most of the signs and symptoms of hypogonadism in males risk of precocious puberty.
(eg, delayed puberty, retention of prepubertal secondary sex In the United States, chorionic gonadotropin has a black-
characteristics after puberty) can be adequately treated with box warning against its use for weight loss. The use of hCG
exogenous androgen; however, treatment of infertility in hypogo- plus severe calorie restriction for weight loss was popularized
nadal men requires the activity of both LH and FSH. For many by a publication in the 1950s claiming that the hCG selectively