
Page 66 - APPENDICES for Fred Falten
P. 66
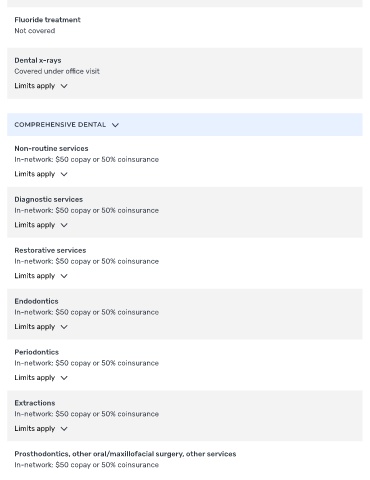
Fluoride treatment
Not covered
Dental x-rays
Covered under o ce visit
Limits apply
COMPREHENSIVE DENTAL
Non-routine services
In-network: $50 copay or 50% coinsurance
Limits apply
Diagnostic services
In-network: $50 copay or 50% coinsurance
Limits apply
Restorative services
In-network: $50 copay or 50% coinsurance
Limits apply
Endodontics
In-network: $50 copay or 50% coinsurance
Limits apply
Periodontics
In-network: $50 copay or 50% coinsurance
Limits apply
Extractions
In-network: $50 copay or 50% coinsurance
Limits apply
Prosthodontics, other oral/maxillofacial surgery, other services
In-network: $50 copay or 50% coinsurance