
Page 85 - APPENDICES for Fred Falten
P. 85
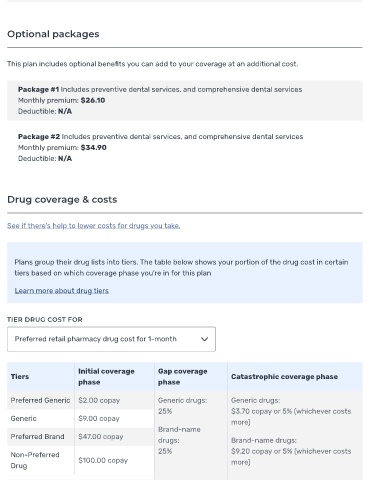
Optional packages
This plan includes optional bene ts you can add to your coverage at an additional cost.
Package #1 Includes preventive dental services, and comprehensive dental services
Monthly premium: $26.10
Deductible: N/A
Package #2 Includes preventive dental services, and comprehensive dental services
Monthly premium: $34.90
Deductible: N/A
Drug coverage & costs
See if there's help to lower costs for drugs you take.
Plans group their drug lists into tiers. The table below shows your portion of the drug cost in certain
tiers based on which coverage phase you're in for this plan
Learn more about drug tiers
TIER DRUG COST FOR
Preferred retail pharmacy drug cost for 1-month
Initial coverage Gap coverage
Tiers Catastrophic coverage phase
phase phase
Preferred Generic $2.00 copay Generic drugs: Generic drugs:
25% $3.70 copay or 5% (whichever costs
Generic $9.00 copay
more)
Brand-name
Preferred Brand $47.00 copay
drugs: Brand-name drugs:
25% $9.20 copay or 5% (whichever costs
Non-Preferred
$100.00 copay more)
Drug