
Page 53 - Cover Letter and Appendices for Melanie April 2019
P. 53
Your Medicare Health Plan Details https://www.medicare.gov/find-a-plan/results/planresults/plan-details.as...
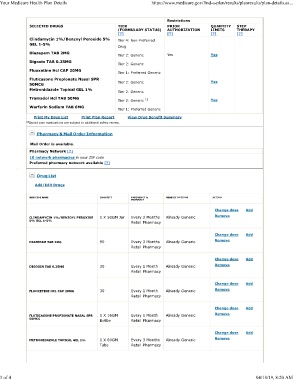
Restrictions
SELECTED DRUGS TIER PRIOR QUANTITY STEP
(FORMULARY STATUS) AUTHORIZATION LIMITS THERAPY
[?] [?] [?] [?]
Clindamycin 1%/Benzoyl Peroxide 5% Tier 4: Non-Preferred
GEL 1-5%
Drug
Diazepam TAB 2MG
Tier 2: Generic Yes Yes
Digoxin TAB 0.25MG
Tier 2: Generic
Fluoxetine Hcl CAP 20MG
Tier 1: Preferred Generic
Fluticasone Propionate Nasal SPR
50MCG Tier 2: Generic Yes
Metronidazole Topical GEL 1%
Tier 2: Generic
Tramadol Hcl TAB 50MG
Tier 2: Generic 13 Yes
Warfarin Sodium TAB 6MG
Tier 1: Preferred Generic
Print My Drug List Print Plan Report View Drug Benefit Summary
13 Opioid pain medications are subject to additional safety review.
Pharmacy & Mail Order Information
Mail Order is available.
Pharmacy Network [?]
10 network pharmacies in your ZIP code
Preferred pharmacy network available [?]
Drug List
Add/Edit Drugs
MEDICINE NAME QUANTITY FREQUENCY & GENERIC OPTIONS ACTION
PHARMACY
Change dose Add
CLINDAMYCIN 1%/BENZOYL PEROXIDE 1 X 50GM Jar Every 2 Months Already Generic Remove
5% GEL 1-5%
Retail Pharmacy
Change dose Add
DIAZEPAM TAB 2MG 90 Every 3 Months Already Generic Remove
Retail Pharmacy
Change dose Add
DIGOXIN TAB 0.25MG 30 Every 1 Month Already Generic Remove
Retail Pharmacy
Change dose Add
FLUOXETINE HCL CAP 20MG 30 Every 1 Month Already Generic Remove
Retail Pharmacy
Change dose Add
FLUTICASONE PROPIONATE NASAL SPR 1 X 16GM Every 1 Month Already Generic Remove
50MCG
Bottle Retail Pharmacy
Change dose Add
METRONIDAZOLE TOPICAL GEL 1% 1 X 60GM Every 3 Months Already Generic Remove
Tube Retail Pharmacy
3 of 4 04/18/19, 8:20 AM