
Page 41 - Memo to Michael Boucher
P. 41
e
v
o
g
a
r
c
i
t
i
l
a
c
r
v
o
e
p
e
G
e
a
a
g
I
Initial coverage Gap coverage
n
g
e
a
r
a
C
h
a
s
p
e
Tiers
T i e r s Catastrophic coverage phase
e
a
p
t
o
t
r
s
c
o
v
h
i
c
s
e
p
a
phase phase
p
h
a
h
e
s
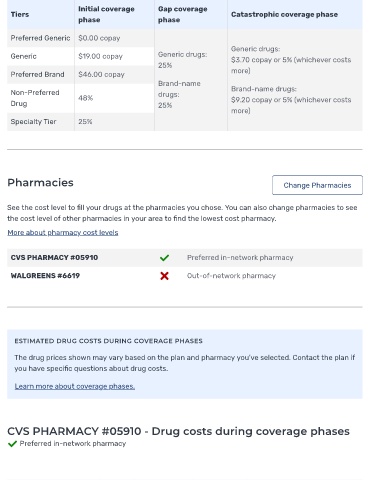
Preferred Generic $0.00 copay
Generic drugs:
Generic $19.00 copay Generic drugs: $3.70 copay or 5% (whichever costs
25%
Preferred Brand $46.00 copay more)
Brand-name
Non-Preferred drugs: Brand-name drugs:
48% $9.20 copay or 5% (whichever costs
Drug 25%
more)
Specialty Tier 25%
Pharmacies Change Pharmacies
See the cost level to ll your drugs at the pharmacies you chose. You can also change pharmacies to see
the cost level of other pharmacies in your area to nd the lowest cost pharmacy.
More about pharmacy cost levels
CVS PHARMACY #05910 Preferred in-network pharmacy
WALGREENS #6619 Out-of-network pharmacy
ESTIMATED DRUG COSTS DURING COVERAGE PHASES
The drug prices shown may vary based on the plan and pharmacy you've selected. Contact the plan if
you have speci c questions about drug costs.
Learn more about coverage phases.
CVS PHARMACY #05910 - Drug costs during coverage phases
Preferred in-network pharmacy