
Page 53 - Evaluation for 2018
P. 53
1/3/2018 Your Medicare Health Plan Details
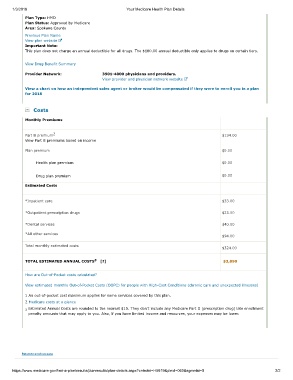
Plan Type: HMO
Plan Status: Approved by Medicare
Area: Spokane County
Previous Plan Name
View plan website
Important Note:
This plan does not charge an annual deductible for all drugs. The $180.00 annual deductible only applies to drugs on certain tiers.
View Drug Benefit Summary
Provider Network: 3501-4000 physicians and providers.
View provider and physician network website
View a chart on how an independent sales agent or broker would be compensated if they were to enroll you in a plan
for 2018
Costs
Monthly Premiums
2
Part B premium $134.00
View Part B premiums based on income
Plan premium $0.00
Health plan premium $0.00
Drug plan premium $0.00
Estimated Costs
*Inpatient care $33.00
*Outpatient prescription drugs $23.00
*Dental services $40.00
*All other services
$94.00
Total monthly estimated costs
$324.00
3
TOTAL ESTIMATED ANNUAL COSTS [?] $3,890
How are Out-of-Pocket costs calculated?
View estimated monthly Out-of-Pocket Costs (OOPC) for people with High-Cost Conditions (chronic care and unexpected illnesses)
1 An out-of-pocket cost maximum applies for some services covered by this plan.
2 Medicare costs at a glance
3 Estimated Annual Costs are rounded to the nearest $10. They don't include any Medicare Part D (prescription drug) late enrollment
penalty amounts that may apply to you. Also, if you have limited income and resources, your expenses may be lower.
Return to previous page
https://www.medicare.gov/find-a-plan/results/planresults/plan-details.aspx?cntrctid=H5619&plnid=060&sgmntid=0 2/2