
Page 75 - Appendices to Jane Miller's evaluation
P. 75
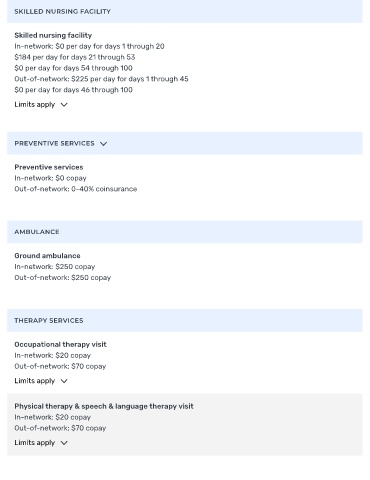
SKILLED NURSING FACILITY
Skilled nursing facility
In-network: $0 per day for days 1 through 20
$184 per day for days 21 through 53
$0 per day for days 54 through 100
Out-of-network: $225 per day for days 1 through 45
$0 per day for days 46 through 100
Limits apply
PREVENTIVE SERVICES
Preventive services
In-network: $0 copay
Out-of-network: 0-40% coinsurance
AMBULANCE
Ground ambulance
In-network: $250 copay
Out-of-network: $250 copay
THERAPY SERVICES
Occupational therapy visit
In-network: $20 copay
Out-of-network: $70 copay
Limits apply
Physical therapy & speech & language therapy visit
In-network: $20 copay
Out-of-network: $70 copay
Limits apply