Page 16 - 2015 Reznor Salary Enrollment Guide
P. 16
Open
Enrollment
Vision Care
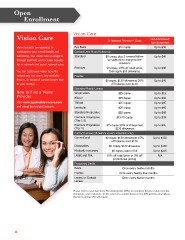
Vision Care In-Network “Member” Costs Out-Of-Network
Reimbursement
Vision beneits are essential to Eye Exam $10 copay Up to $30
maintaining your overall health and Contact Lens it and follow-up
well-being. Our vision care coverage is Standard $0 copay, plus 2 covered follow Up to $40
through EyeMed, and includes beneits up visits at no charge to the
for in-network and out of network care . employee
Premium $0 copay, 10% off retail price, Up to $40
You can apply your vision beneits then apply $55 allowance
toward any eye exam, any available Frames
frames, or brand of contact lenses that $0 copay, $130 allowance; 20% Up to $40
it your lifestyle. off balance over $130
Standard Plastic Lenses
How to Find a Vision Single vision $25 copay Up to $15
Provider Bifocal $25 copay Up to $30
Visit www.eyemedvisioncare.com Trifocal $25 copay Up to $45
and select the Insight Network. Lenticular $25 copay Up to $45
Standard Progressive $25 copay Up to $45
Premium Progressive $45-70 copay Up to $45
(Tier 1-3)
Premium Progressive $25 copay 80% of charge less Up to $45
(Tier 4) $120 allowance
Contact Lenses (allowance covers materials only)
Conventional $0 copay, $130 allowance; 15% Up to $130
off balance over $130
Disposables $0 copay, $130 allowance Up to $130
Medically necessary $0 copay; paid in full Up to $210
LASIK and PRK 15% off retail price or 5% off N/A
promotional pricing
Frequency Limits
Exam Once every twelve months
Frames Once every twenty four months
Lenses or Contact Once every twelve months
Lenses
Please refer to your Summary Plan Description (SPD) for complete details of plan beneits,
limitations, and exclusions. In the event of a conlict between the SPD and this description,
the terms of the SPD will prevail.
16
Enrollment
Vision Care
Vision Care In-Network “Member” Costs Out-Of-Network
Reimbursement
Vision beneits are essential to Eye Exam $10 copay Up to $30
maintaining your overall health and Contact Lens it and follow-up
well-being. Our vision care coverage is Standard $0 copay, plus 2 covered follow Up to $40
through EyeMed, and includes beneits up visits at no charge to the
for in-network and out of network care . employee
Premium $0 copay, 10% off retail price, Up to $40
You can apply your vision beneits then apply $55 allowance
toward any eye exam, any available Frames
frames, or brand of contact lenses that $0 copay, $130 allowance; 20% Up to $40
it your lifestyle. off balance over $130
Standard Plastic Lenses
How to Find a Vision Single vision $25 copay Up to $15
Provider Bifocal $25 copay Up to $30
Visit www.eyemedvisioncare.com Trifocal $25 copay Up to $45
and select the Insight Network. Lenticular $25 copay Up to $45
Standard Progressive $25 copay Up to $45
Premium Progressive $45-70 copay Up to $45
(Tier 1-3)
Premium Progressive $25 copay 80% of charge less Up to $45
(Tier 4) $120 allowance
Contact Lenses (allowance covers materials only)
Conventional $0 copay, $130 allowance; 15% Up to $130
off balance over $130
Disposables $0 copay, $130 allowance Up to $130
Medically necessary $0 copay; paid in full Up to $210
LASIK and PRK 15% off retail price or 5% off N/A
promotional pricing
Frequency Limits
Exam Once every twelve months
Frames Once every twenty four months
Lenses or Contact Once every twelve months
Lenses
Please refer to your Summary Plan Description (SPD) for complete details of plan beneits,
limitations, and exclusions. In the event of a conlict between the SPD and this description,
the terms of the SPD will prevail.
16