Page 11 - 2015 Advia CU Benefits & Notices
P. 11
Advia CU - MI 2015
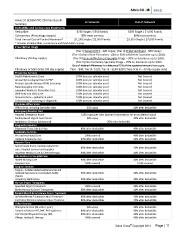
Advia CU BCBSM PPO 250 Plan Benefit In Network Out-of-Network
Summary
Deductible and Coinsurance Maximums
Deductible $250 Single / $500 Family $500 Single / $1,000 Family
Coinsurance (Percentage copays) 80% most services 60% most services
Total Annual Out-of-Pocket Maximum* $1,250 Single / $2,500 Family $3,500 Single / $7,000 Family
* Includes all deductible, co-insurance and fixed dollar co-pays.
Prescription Drugs
(Tier I) Generic/OTC - $20 copay; (Tier II) Preferred Brand - $60 copay;
(Tier III) Brand Non-Formulary - $80 or 50% whichever is greater up to $100;
Pharmacy (30 day supply) (Tier IV) Generic/Preferred Specialty Drugs – 20% co-insurance up to $200;
(Tier V) Non-formulary Specialty Drugs – 25% co-insurance up to $300
Out-of-Network Pharmacy is reimbursed 75% of the approved amount less copay.
Pharmacy or Mail Order (90 day supply) Tier I - $40; Tier II - $120; Tier III - $160-$200 (Tiers IV & V – 30 day supply only)
Preventive Services
Health Maintenance Exam 100% (one per calendar year) Not Covered
Annual Gynecological Exam & PAP 100% (one per calendar year) Not Covered
Prostate Specific Antigen (PSA) Screening 100% (one per calendar year) Not Covered
Mammography Screening 100% (one per calendar year) Not Covered
Expanded Women’s Preventive Care 100% (one per calendar year) Not Covered
Well-Baby and Child Care 100% (one per calendar year) Not Covered
Immunizations – pediatric & adult 100% (one per calendar year) Not Covered
Colonoscopy – screening or diagnostic 100% (one per calendar year) Not Covered
Physician Office Visits
Office visits, including Specialist visits $20 copay 40% after deductible
Emergency Medical Care
Hospital Emergency Room $150 copay per visits (waived if admitted or for an accidental injury)
Facility Based Urgent Care Center $20 copay 40% after deductible
Ambulance Services (air/ground) 20% after deductible
Diagnostic Services
Diagnostic Tests, Lab & X-Ray 80% after deductible 40% after deductible
Maternity Services
Pre and Post-natal Care 100% covered 40% after deductible
Delivery & Nursery Care 80% after deductible 40% after deductible
Hospital Care
Semi-Private Room, Inpatient physician 80% after deductible 40% after deductible
care, Hospital services and supplies
Inpatient Medical Care & Chemotherapy 80% after deductible 40% after deductible
Alternatives to Hospital Care
Skilled Nursing Care 80% after deductible 40% after deductible
Hospice Care 100% covered 100% covered
Surgical Services
Surgery – includes related surgical services and 80% after deductible 40% after deductible
medically necessary in or out-patient facility
charges
Voluntary Sterilization 80% after deductible 40% after deductible
Human Organ Transplants
Specified Organ Transplants 100% covered 40% after deductible
Bone Marrow & Other Transplants 80% after deductible 40% after deductible
Mental Health & Substance Abuse Treatment
In Patient Mental & Substance Abuse Treatment 80% after deductible 40% after deductible
Out Patient Mental & Substance Abuse Treatment 80% after deductible 40% after deductible
Other Services
Chiropractic Care (24 visits / year) $20 copay 40% after deductible
Outpatient Diabetes MT, DME, P&O appliances 80% after deductible 40% after deductible
O/P Occ/SP/Physical Therapy (60) 80% after deductible 40% after deductible
Allergy Testing & Therapy 100% covered 40% after deductible
Salus Group© Copyright 2014 Page | 11
Advia CU BCBSM PPO 250 Plan Benefit In Network Out-of-Network
Summary
Deductible and Coinsurance Maximums
Deductible $250 Single / $500 Family $500 Single / $1,000 Family
Coinsurance (Percentage copays) 80% most services 60% most services
Total Annual Out-of-Pocket Maximum* $1,250 Single / $2,500 Family $3,500 Single / $7,000 Family
* Includes all deductible, co-insurance and fixed dollar co-pays.
Prescription Drugs
(Tier I) Generic/OTC - $20 copay; (Tier II) Preferred Brand - $60 copay;
(Tier III) Brand Non-Formulary - $80 or 50% whichever is greater up to $100;
Pharmacy (30 day supply) (Tier IV) Generic/Preferred Specialty Drugs – 20% co-insurance up to $200;
(Tier V) Non-formulary Specialty Drugs – 25% co-insurance up to $300
Out-of-Network Pharmacy is reimbursed 75% of the approved amount less copay.
Pharmacy or Mail Order (90 day supply) Tier I - $40; Tier II - $120; Tier III - $160-$200 (Tiers IV & V – 30 day supply only)
Preventive Services
Health Maintenance Exam 100% (one per calendar year) Not Covered
Annual Gynecological Exam & PAP 100% (one per calendar year) Not Covered
Prostate Specific Antigen (PSA) Screening 100% (one per calendar year) Not Covered
Mammography Screening 100% (one per calendar year) Not Covered
Expanded Women’s Preventive Care 100% (one per calendar year) Not Covered
Well-Baby and Child Care 100% (one per calendar year) Not Covered
Immunizations – pediatric & adult 100% (one per calendar year) Not Covered
Colonoscopy – screening or diagnostic 100% (one per calendar year) Not Covered
Physician Office Visits
Office visits, including Specialist visits $20 copay 40% after deductible
Emergency Medical Care
Hospital Emergency Room $150 copay per visits (waived if admitted or for an accidental injury)
Facility Based Urgent Care Center $20 copay 40% after deductible
Ambulance Services (air/ground) 20% after deductible
Diagnostic Services
Diagnostic Tests, Lab & X-Ray 80% after deductible 40% after deductible
Maternity Services
Pre and Post-natal Care 100% covered 40% after deductible
Delivery & Nursery Care 80% after deductible 40% after deductible
Hospital Care
Semi-Private Room, Inpatient physician 80% after deductible 40% after deductible
care, Hospital services and supplies
Inpatient Medical Care & Chemotherapy 80% after deductible 40% after deductible
Alternatives to Hospital Care
Skilled Nursing Care 80% after deductible 40% after deductible
Hospice Care 100% covered 100% covered
Surgical Services
Surgery – includes related surgical services and 80% after deductible 40% after deductible
medically necessary in or out-patient facility
charges
Voluntary Sterilization 80% after deductible 40% after deductible
Human Organ Transplants
Specified Organ Transplants 100% covered 40% after deductible
Bone Marrow & Other Transplants 80% after deductible 40% after deductible
Mental Health & Substance Abuse Treatment
In Patient Mental & Substance Abuse Treatment 80% after deductible 40% after deductible
Out Patient Mental & Substance Abuse Treatment 80% after deductible 40% after deductible
Other Services
Chiropractic Care (24 visits / year) $20 copay 40% after deductible
Outpatient Diabetes MT, DME, P&O appliances 80% after deductible 40% after deductible
O/P Occ/SP/Physical Therapy (60) 80% after deductible 40% after deductible
Allergy Testing & Therapy 100% covered 40% after deductible
Salus Group© Copyright 2014 Page | 11