Page 8 - 2015 Advia CU Open Enrollment PPT
P. 8
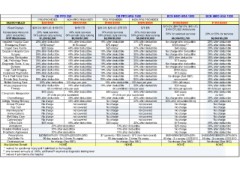
CB PPO 250 CB PPO HRA 1500 BCN HMO HRA 1000 BCN HMO HSA 1300
PPO PROVIDER NON-PPO PROVIDER PPO PROVIDER NON-PPO PROVIDER $1000/$2000 $1300/$2600
DEDUCTIBLES $250/$500 $500/$1000 $1500/$3000 $3000/$6000 $15 OV; $30 Ref OV; $45 UC; 20% or 50% for services
$100 ER; $25 Ambulance
Fixed Copays $20 OV; $20 UC; $150 ER $150 ER $20 OV; $20 UC; $75 ER $75 ER $2,600/$5,200
50% for selected services 20% after deductible
Coinsurance Amounts 20% most services 40% most services 10% most services 30% most services 20% after deductible
(after deductible) 50% private duty nursing 50% private duty nursing $6,350/$12,700 20% after deductible
OOP Maximums 50% private duty nursing 50% private duty nursing 20% after deductible
$1,250/$2,500 $3,500/$7,000 No charge after deductible 20% after deductible
$2,500/$5,000 $5,000/$10,000 $100 copay*** 50% after deductible
$45 copay 20% after deductible
Inpatient Hospital Care 20% after deductible 40% after deductible 10% after deductible 30% after deductible 20% after deductible
Emergency Room No charge after deductible 20% after deductible
Urgent Care Facility $150 copay* $150 copay* $75 copay* $75 copay* No charge after deductible 20% after deductible
20% after deductible
Outpatient Hospital Care $20 copay 40% after deductible $20 copay 30% after deductible 50% after deductible 20% after deductible
Surgery $15 copay 20% after deductible
20% after deductible 40% after deductible 10% after deductible 30% after deductible 20% after deductible
Voluntary Sterilization No charge after deductible 20% after deductible
Lab, Pathology Tests 20% after deductible 40% after deductible 10% after deductible 30% after deductible No charge after deductible 60 visits per episode
Diagnostic Tests, X-ray 20% after deductible
20% after deductible 40% after deductible 10% after deductible 30% after deductible $150 copay
Delivery $15 copay no limit
High Tech Imaging 20% after deductible 40% after deductible 10% after deductible 30% after deductible No charge (See SBC) 20% after deductible
Outpatient Psychiatric not covered 20% after deductible
Pre & Post Natal Care 20% after deductible 40% after deductible 10% after deductible 30% after deductible 100% (45 days)
Private Duty Nursing $30 copay No charge
Skilled Nursing Care 20% after deductible 40% after deductible 10% after deductible 30% after deductible 60 visits per episode No charge
Physical/Speech/Occ $30 copay No charge
20% after deductible 40% after deductible 10% after deductible 30% after deductible No charge
Therapy no limit No charge
20% after deductible 40% after deductible 10% after deductible 30% after deductible No charge after deductible No charge
Chiropractic Manipulation 50% after deductible/$5 inj 20% after deductible
No charge 40% after deductible 10% after deductible 30% after deductible 20% after deductible
Chemotherapy No charge 50% after deductible
Allergy Testing/Therapy 50% after deductible 50% after deductible 50% after deductible 50% after deductible No charge 50% after deductible
No charge $4/$15/$40/$80/20%/20%/50%
Annual Physical 20% after deductible – 120 days per year 10% after deductible – 120 days per year No charge 90 day - 3 x co-pay LESS $10
Pap Test No charge No charge (See SBC)
20% after deductible 40% after deductible 10% after deductible 30% after deductible No charge
Mammograms** $15 copay NONE
Immunizations 60 combined visits per year 60 combined visits per year $25 copay
Well Baby Care No charge
Colonoscopy** $20 copay 40% after deductible $20 copay 30% after deductible No charge
$6/$40/$60/$80/20%/20%
Office Calls 24 visits per year (combined) 24 visits per year (combined) 90 day - 3 x co-pay LESS $10
Ambulance No charge (See SBC)
Durable Medical Equip 20% after deductible 40% after deductible 10% after deductible 30% after deductible
Prosthetic Appliances NONE
Prescriptions No charge 40% after deductible No charge 30% after deductible
Mail Order Rx
Contraceptives No charge not covered No charge not covered
Max Lifetime Benefit
No charge not covered No charge not covered
No charge not covered No charge not covered
No charge not covered No charge not covered
No charge not covered No charge not covered
No charge not covered No charge not covered
$20 copay 40% after deductible $20 copay 30% after deductible
20% after deductible 10% after deductible
20% after deductible 10% after deductible
20% after deductible 10% after deductible
$20/$60/50%(80-100)/20%(200)/20%(300) $7 (generic) / $35 (brand) / $70 (non-form brand)
90 day supply for 2 times Rx copay 90 day supply for 2 times Rx copay
No charge (See SBC) No charge (See SBC)
NONE NONE
* waived for accidental injury and if admitted to the hospital
** one covered annually at 100%; additional if required at diagnostic testing level
*** waived if admitted to the hospital
PPO PROVIDER NON-PPO PROVIDER PPO PROVIDER NON-PPO PROVIDER $1000/$2000 $1300/$2600
DEDUCTIBLES $250/$500 $500/$1000 $1500/$3000 $3000/$6000 $15 OV; $30 Ref OV; $45 UC; 20% or 50% for services
$100 ER; $25 Ambulance
Fixed Copays $20 OV; $20 UC; $150 ER $150 ER $20 OV; $20 UC; $75 ER $75 ER $2,600/$5,200
50% for selected services 20% after deductible
Coinsurance Amounts 20% most services 40% most services 10% most services 30% most services 20% after deductible
(after deductible) 50% private duty nursing 50% private duty nursing $6,350/$12,700 20% after deductible
OOP Maximums 50% private duty nursing 50% private duty nursing 20% after deductible
$1,250/$2,500 $3,500/$7,000 No charge after deductible 20% after deductible
$2,500/$5,000 $5,000/$10,000 $100 copay*** 50% after deductible
$45 copay 20% after deductible
Inpatient Hospital Care 20% after deductible 40% after deductible 10% after deductible 30% after deductible 20% after deductible
Emergency Room No charge after deductible 20% after deductible
Urgent Care Facility $150 copay* $150 copay* $75 copay* $75 copay* No charge after deductible 20% after deductible
20% after deductible
Outpatient Hospital Care $20 copay 40% after deductible $20 copay 30% after deductible 50% after deductible 20% after deductible
Surgery $15 copay 20% after deductible
20% after deductible 40% after deductible 10% after deductible 30% after deductible 20% after deductible
Voluntary Sterilization No charge after deductible 20% after deductible
Lab, Pathology Tests 20% after deductible 40% after deductible 10% after deductible 30% after deductible No charge after deductible 60 visits per episode
Diagnostic Tests, X-ray 20% after deductible
20% after deductible 40% after deductible 10% after deductible 30% after deductible $150 copay
Delivery $15 copay no limit
High Tech Imaging 20% after deductible 40% after deductible 10% after deductible 30% after deductible No charge (See SBC) 20% after deductible
Outpatient Psychiatric not covered 20% after deductible
Pre & Post Natal Care 20% after deductible 40% after deductible 10% after deductible 30% after deductible 100% (45 days)
Private Duty Nursing $30 copay No charge
Skilled Nursing Care 20% after deductible 40% after deductible 10% after deductible 30% after deductible 60 visits per episode No charge
Physical/Speech/Occ $30 copay No charge
20% after deductible 40% after deductible 10% after deductible 30% after deductible No charge
Therapy no limit No charge
20% after deductible 40% after deductible 10% after deductible 30% after deductible No charge after deductible No charge
Chiropractic Manipulation 50% after deductible/$5 inj 20% after deductible
No charge 40% after deductible 10% after deductible 30% after deductible 20% after deductible
Chemotherapy No charge 50% after deductible
Allergy Testing/Therapy 50% after deductible 50% after deductible 50% after deductible 50% after deductible No charge 50% after deductible
No charge $4/$15/$40/$80/20%/20%/50%
Annual Physical 20% after deductible – 120 days per year 10% after deductible – 120 days per year No charge 90 day - 3 x co-pay LESS $10
Pap Test No charge No charge (See SBC)
20% after deductible 40% after deductible 10% after deductible 30% after deductible No charge
Mammograms** $15 copay NONE
Immunizations 60 combined visits per year 60 combined visits per year $25 copay
Well Baby Care No charge
Colonoscopy** $20 copay 40% after deductible $20 copay 30% after deductible No charge
$6/$40/$60/$80/20%/20%
Office Calls 24 visits per year (combined) 24 visits per year (combined) 90 day - 3 x co-pay LESS $10
Ambulance No charge (See SBC)
Durable Medical Equip 20% after deductible 40% after deductible 10% after deductible 30% after deductible
Prosthetic Appliances NONE
Prescriptions No charge 40% after deductible No charge 30% after deductible
Mail Order Rx
Contraceptives No charge not covered No charge not covered
Max Lifetime Benefit
No charge not covered No charge not covered
No charge not covered No charge not covered
No charge not covered No charge not covered
No charge not covered No charge not covered
No charge not covered No charge not covered
$20 copay 40% after deductible $20 copay 30% after deductible
20% after deductible 10% after deductible
20% after deductible 10% after deductible
20% after deductible 10% after deductible
$20/$60/50%(80-100)/20%(200)/20%(300) $7 (generic) / $35 (brand) / $70 (non-form brand)
90 day supply for 2 times Rx copay 90 day supply for 2 times Rx copay
No charge (See SBC) No charge (See SBC)
NONE NONE
* waived for accidental injury and if admitted to the hospital
** one covered annually at 100%; additional if required at diagnostic testing level
*** waived if admitted to the hospital