
Page 65 - Benefits Summary 2018-2019
P. 65
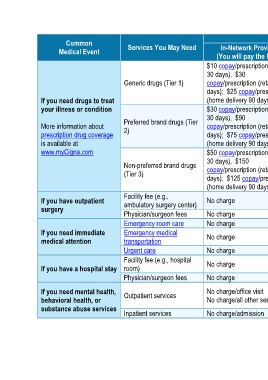
What You Will Pay
Common Services You May Need Limitations, Exceptions, & Other
Medical Event In-Network Provider Out-of-Network Provider Important Information
(You will pay the least) (You will pay the most)
$10 copay/prescription (retail
30 days), $30 50% coinsurance/prescription
Generic drugs (Tier 1) copay/prescription (retail 90 (retail); Not covered (home
days); $25 copay/prescription delivery)
If you need drugs to treat (home delivery 90 days) Coverage is limited up to a 90-day
your illness or condition $30 copay/prescription (retail supply (retail and home delivery); up
30 days), $90 50% coinsurance/prescription to a 30-day supply (retail and home
Preferred brand drugs (Tier delivery) for Specialty drugs.
More information about copay/prescription (retail 90 (retail); Not covered (home
prescription drug coverage 2) days); $75 copay/prescription delivery) Certain limitations may apply,
is available at (home delivery 90 days) including, for example: prior
www.myCigna.com $50 copay/prescription (retail authorization, step therapy, quantity
limits.
30 days), $150 50% coinsurance/prescription
Non-preferred brand drugs copay/prescription (retail 90 (retail); Not covered (home
(Tier 3)
days); $125 copay/prescription delivery)
(home delivery 90 days)
Facility fee (e.g.,
If you have outpatient ambulatory surgery center) No charge 30% coinsurance $250 penalty for no precertification.
surgery
Physician/surgeon fees No charge 30% coinsurance $250 penalty for no precertification.
Emergency room care No charge No charge None
If you need immediate Emergency medical No charge No charge None
medical attention transportation
Urgent care No charge 30% coinsurance None
Facility fee (e.g., hospital
If you have a hospital stay room) No charge 30% coinsurance $250 penalty for no precertification.
Physician/surgeon fees No charge 30% coinsurance $250 penalty for no precertification.
30% coinsurance/office visit $250 penalty if no precert of non-
If you need mental health, Outpatient services No charge/office visit 30% coinsurance/all other routine services (i.e., partial
behavioral health, or No charge/all other services services hospitalization, IOP, etc.).
substance abuse services
Inpatient services No charge/admission 30% coinsurance $250 penalty for no precertification.
3 of 7