
Page 100 - Tampa Bay Rays 2022 Flipbook
P. 100
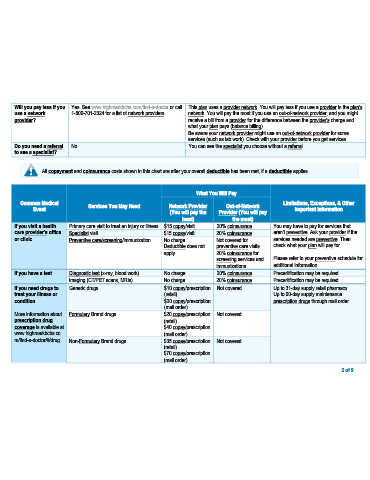
Will you pay less if you Yes. See www.highmarkbcbs.com/find-a-doctor or call This plan uses a provider network. You will pay less if you use a provider in the plan’s
use a network 1-800-701-2324 for a list of network providers. network. You will pay the most if you use an out-of-network provider, and you might
provider? receive a bill from a provider for the difference between the provider’s charge and
what your plan pays (balance billing).
Be aware your network provider might use an out-of-network provider for some
services (such as lab work). Check with your provider before you get services.
Do you need a referral No. You can see the specialist you choose without a referral.
to see a specialist?
All copayment and coinsurance costs shown in this chart are after your overall deductible has been met, if a deductible applies.
What You Will Pay
Common Medical Services You May Need Network Provider Out-of-Network Limitations, Exceptions, & Other
Event Important Information
(You will pay the Provider (You will pay
least) the most)
If you visit a health Primary care visit to treat an injury or illness $15 copay/visit 20% coinsurance You may have to pay for services that
care provider’s office Specialist visit $15 copay/visit 20% coinsurance aren’t preventive. Ask your provider if the
or clinic Preventive care/screening/immunization No charge Not covered for services needed are preventive. Then
Deductible does not preventive care visits check what your plan will pay for.
apply. 20% coinsurance for
screening services and Please refer to your preventive schedule for
immunizations additional information.
If you have a test Diagnostic test (x-ray, blood work) No charge 20% coinsurance Precertification may be required.
Imaging (CT/PET scans, MRIs) No charge 20% coinsurance Precertification may be required.
If you need drugs to Generic drugs $10 copay/prescription Not covered Up to 31-day supply retail pharmacy.
treat your illness or (retail) Up to 90-day supply maintenance
condition $20 copay/prescription prescription drugs through mail order.
(mail order)
More information about Formulary Brand drugs $20 copay/prescription Not covered
prescription drug (retail)
coverage is available at $40 copay/prescription
www.highmarkbcbs.co (mail order)
m/find-a-doctor/#/drug. Non-Formulary Brand drugs $35 copay/prescription Not covered
(retail)
$70 copay/prescription
(mail order)
2 of 9