
Page 194 - 2021 Miami Marlins Front Office Benefits Guide
P. 194
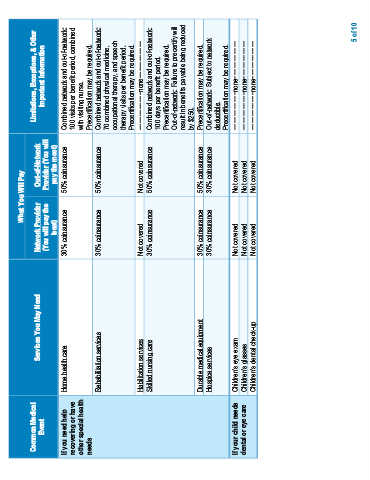
What You Will Pay
Common Medical Services You May Need Network Provider Out-of-Network Limitations, Exceptions, & Other
Event Important Information
(You will pay the Provider (You will
least) pay the most)
If you need help Home health care 30% coinsurance 50% coinsurance Combined network and out-of-network:
recovering or have 100 visits per benefit period, combined
other special health with visiting nurse.
needs Precertification may be required.
Rehabilitation services 30% coinsurance 50% coinsurance Combined network and out-of-network:
70 combined physical medicine,
occupational therapy, and speech
therapy visits per benefit period.
Precertification may be required.
Habilitation services Not covered Not covered −−−−−−−−−−−none−−−−−−−−−−−
Skilled nursing care 30% coinsurance 50% coinsurance Combined network and out-of-network:
100 days per benefit period.
Precertification may be required.
Out-of-network: Failure to precertify will
result in benefits payable being reduced
by $250.
Durable medical equipment 30% coinsurance 50% coinsurance Precertification may be required.
Hospice services 30% coinsurance 30% coinsurance Out-of-network: Subject to network
deductible.
Precertification may be required.
If your child needs Children’s eye exam Not covered Not covered −−−−−−−−−−−none−−−−−−−−−−−
dental or eye care Children’s glasses Not covered Not covered −−−−−−−−−−−none−−−−−−−−−−−
Children’s dental check-up Not covered Not covered −−−−−−−−−−−none−−−−−−−−−−−
5 of 10