
Page 3 - Demo IPC benefits flip
P. 3
®
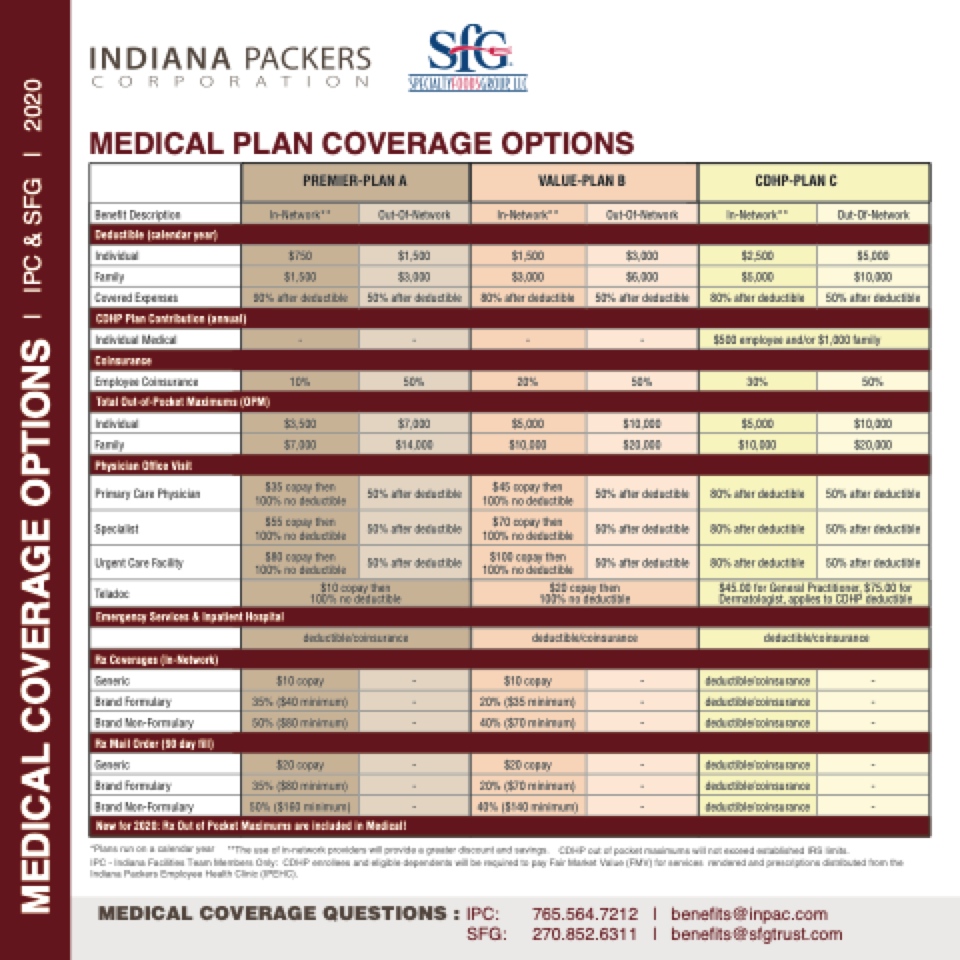
MEDICAL PLAN COVERAGE OPTIONS
CDHP Plan Contribution (annual)
CDHP-PLAN C
Out-Of-Network
$5,000 $10,000
50% after deductible
8$05%00aeftmerpdloeydeuectainbdle/or $15,0%00affatmerildyeductible
50%
$10,000 $20,000
50% after deductible
50% after deductible
50% after deductible
$45.00 for General Practitioner, $75.00 for Dermatologist, applies to CDHP deductible
deductible/coinsurance
- - -
- - -
IPC - Indiana Facilities Team Members Only: CDHP enrollees and eligible dependents will be required to pay Fair Market Value (FMV) for services rendered and prescriptions distributed from the Indiana Packers Employee Health Clinic (IPEHC).
Deductible (calendar year)
PREMIER-PLAN A
VALUE-PLAN B
Benefit Description
In-Network**
Out-Of-Network
In-Network**
Out-Of-Network
In-Network**
Individual
$750
$1,500
$1,500
$3,000
$2,500
Family
$1,500
$3,000
$3,000
$6,000
$5,000
Covered Expenses
90% after deductible
50% after deductible
80% after deductible
50% after deductible
80% after deductible
Individual Medical
Coinsurance
-
-
-
-
Employee Coinsurance
10%
50%
20%
50%
30%
Total Out-of-Pocket Maximums (OPM)
Individual
$3,500
$7,000
$5,000
$10,000
$5,000
Family
$7,000
$14,000
$10,000
$20,000
$10,000
Physician Office Visit
Primary Care Physician
$35 copay then 100% no deductible
50% after deductible
$45 copay then 100% no deductible
50% after deductible
80% after deductible
Specialist
$55 copay then 100% no deductible
50% after deductible
$70 copay then 100% no deductible
50% after deductible
80% after deductible
Urgent Care Facility
$80 copay then 100% no deductible
50% after deductible
$100 copay then 100% no deductible
50% after deductible
80% after deductible
Teladoc
$10 copay then 100% no deductible
$20 copay then 100% no deductible
Emergency Services & Inpatient Hospital
Rx Coverages (In-Network)
deductible/coinsurance
deductible/coinsurance
Generic
$10 copay
-
$10 copay
-
deductible/coinsurance
Brand Formulary
35% ($40 minimum)
-
20% ($35 minimum)
-
deductible/coinsurance
Brand Non-Formulary
50% ($80 minimum)
-
40% ($70 minimum)
-
deductible/coinsurance
Rx Mail Order (90 day fill)
Generic
$20 copay
-
$20 copay
-
deductible/coinsurance
Brand Formulary
35% ($80 minimum)
-
20% ($70 minimum)
-
deductible/coinsurance
Brand Non-Formulary
50% ($160 minimum)
-
40% ($140 minimum)
-
deductible/coinsurance
New for 2020: Rx Out of Pocket Maximums are included in Medical!
*Plans run on a calendar year **The use of in-network providers will provide a greater discount and savings. CDHP out of pocket maximums will not exceed established IRS limits.
MEDICAL COVERAGE QUESTIONS : IPC: 765.564.7212 | benefits@inpac.com SFG: 270.852.6311 | benefits@sfgtrust.com
MEDICAL COVERAGE OPTIONS
| IPC & SFG | 2020
