
Page 5 - Demo IPC benefits flip
P. 5
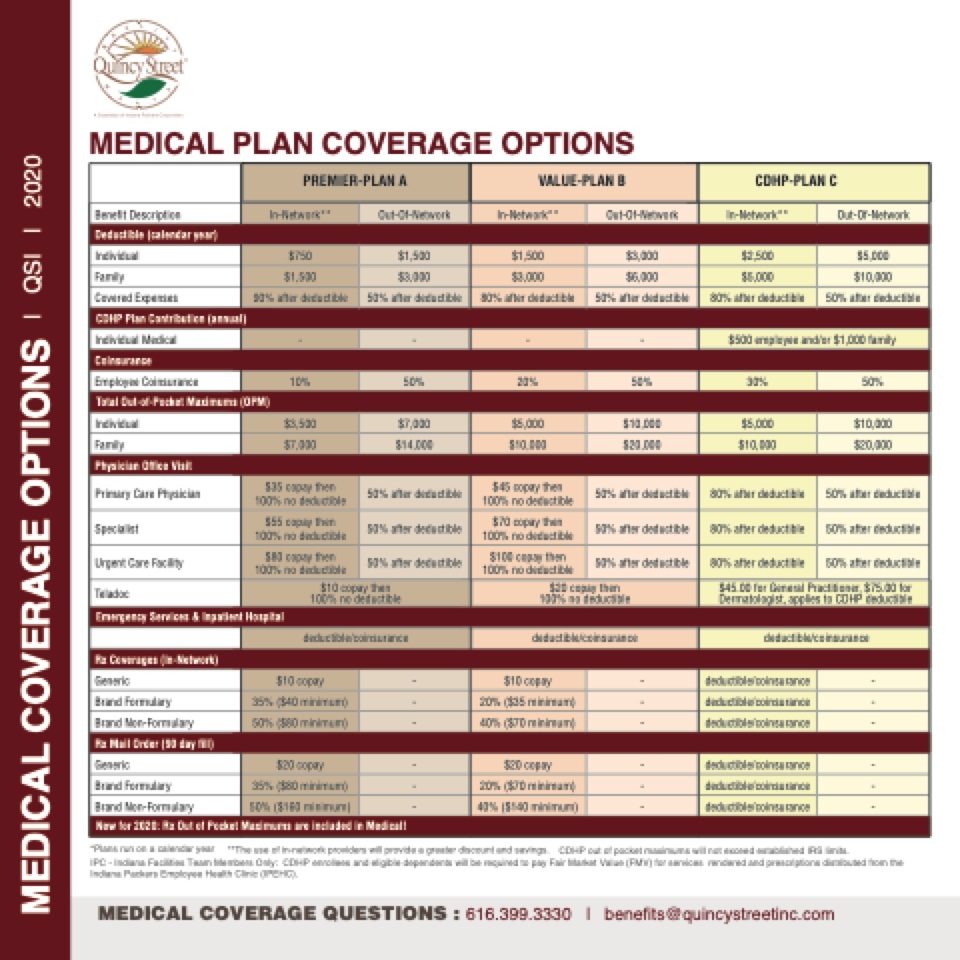
MEDICAL PLAN COVERAGE OPTIONS
CDHP Plan Contribution (annual)
CDHP-PLAN C
Out-Of-Network
$5,000 $10,000
50% after deductible
80%$a5f0te0redmedpulocyteibeleand/o5r 0$%1,0a0ft0erfadmediluyctible
50%
$10,000 $20,000
50% after deductible
50% after deductible
50% after deductible
$45.00 for General Practitioner, $75.00 for Dermatologist, applies to CDHP deductible
deductible/coinsurance
- - -
- - -
IPC - Indiana Facilities Team Members Only: CDHP enrollees and eligible dependents will be required to pay Fair Market Value (FMV) for services rendered and prescriptions distributed from the Indiana Packers Employee Health Clinic (IPEHC).
PREMIER-PLAN A
Benefit Description
In-Network**
Out-Of-Network
In-Network**
Deductible (calendar year)
Individual
$750
$1,500
$1,500
$3,000
$2,500
$3,000
Employee Coinsurance
10%
20%
30%
Total Out-of-Pocket Maximums (OPM)
Individual
$3,500
$7,000
$5,000
$10,000
$5,000
Family
$7,000
$14,000
$10,000
$20,000
$10,000
Physician Office Visit
Primary Care Physician
$35 copay then 100% no deductible
50% after deductible
$45 copay then 100% no deductible
50% after deductible
80% after deductible
Specialist
$55 copay then 100% no deductible
50% after deductible
$70 copay then 100% no deductible
50% after deductible
80% after deductible
Urgent Care Facility
$80 copay then 100% no deductible
50% after deductible
$100 copay then 100% no deductible
50% after deductible
80% after deductible
Teladoc
$10 copay then 100% no deductible
$20 copay then 100% no deductible
Emergency Services & Inpatient Hospital
Generic
deductible/coinsurance
deductible/coinsurance
Rx Coverages (In-Network)
$10 copay
-
$10 copay
-
deductible/coinsurance
Brand Formulary
35% ($40 minimum)
-
20% ($35 minimum)
-
deductible/coinsurance
Brand Non-Formulary
50% ($80 minimum)
-
40% ($70 minimum)
-
deductible/coinsurance
Rx Mail Order (90 day fill)
Generic
$20 copay
-
$20 copay
-
deductible/coinsurance
Brand Formulary
35% ($80 minimum)
-
20% ($70 minimum)
-
deductible/coinsurance
Brand Non-Formulary
50% ($160 minimum)
-
40% ($140 minimum)
-
deductible/coinsurance
New for 2020: Rx Out of Pocket Maximums are included in Medical!
*Plans run on a calendar year **The use of in-network providers will provide a greater discount and savings. CDHP out of pocket maximums will not exceed established IRS limits.
In-Network**
VALUE-PLAN B
Out-Of-Network
Family
$1,500
$3,000
$6,000
$5,000
Covered Expenses
90% after deductible
50% after deductible
80% after deductible
50% after deductible
80% after deductible
Individual Medical
-
-
-
-
Coinsurance
50%
50%
MEDICAL COVERAGE QUESTIONS : 616.399.3330 | benefits@quincystreetinc.com
MEDICAL COVERAGE OPTIONS
| QSI | 2020
