
Page 5 - Playmakers 2020 Renewal Benefits Booklet
P. 5
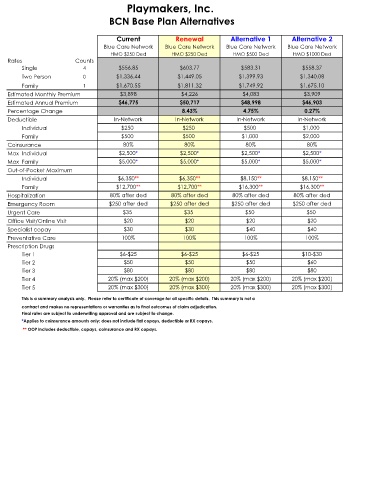
Playmakers, Inc.
BCN Base Plan Alternatives
Current Renewal Alternative 1 Alternative 2
Blue Care Network Blue Care Network Blue Care Network Blue Care Network
HMO $250 Ded HMO $250 Ded HMO $500 Ded HMO $1000 Ded
Rates Counts
Single 4 $556.85 $603.77 $583.31 $558.37
Two Person 0 $1,336.44 $1,449.05 $1,399.93 $1,340.08
Family 1 $1,670.55 $1,811.32 $1,749.92 $1,675.10
Estimated Monthly Premium $3,898 $4,226 $4,083 $3,909
Estimated Annual Premium $46,775 $50,717 $48,998 $46,903
Percentage Change 8.43% 4.75% 0.27%
Deductible In-Network In-Network In-Network In-Network
Individual $250 $250 $500 $1,000
Family $500 $500 $1,000 $2,000
Coinsurance 80% 80% 80% 80%
Max Individual $2,500* $2,500* $2,500* $2,500*
Max Family $5,000* $5,000* $5,000* $5,000*
Out-of-Pocket Maximum
Individual $6,350** $6,350** $8,150** $8,150**
Family $12,700** $12,700** $16,300** $16,300**
Hospitalization 80% after ded 80% after ded 80% after ded 80% after ded
Emergency Room $250 after ded $250 after ded $250 after ded $250 after ded
Urgent Care $35 $35 $50 $50
Office Visit/Online Visit $20 $20 $20 $20
Specialist copay $30 $30 $40 $40
Preventative Care 100% 100% 100% 100%
Prescription Drugs
Tier 1 $6-$25 $6-$25 $6-$25 $10-$30
Tier 2 $50 $50 $50 $60
Tier 3 $80 $80 $80 $80
Tier 4 20% (max $200) 20% (max $200) 20% (max $200) 20% (max $200)
Tier 5 20% (max $300) 20% (max $300) 20% (max $300) 20% (max $300)
This is a summary analysis only. Please refer to certificate of coverage for all specific details. This summary is not a
contract and makes no representations or warranties as to final outcomes of claim adjudication.
Final rates are subject to underwriting approval and are subject to change.
*Applies to coinsurance amounts only; does not include flat copays, deductible or RX copays.
** OOP includes deductible, copays, coinsurance and RX copays.