
Page 5 - Canada Dry Bottling Renewal 2020
P. 5
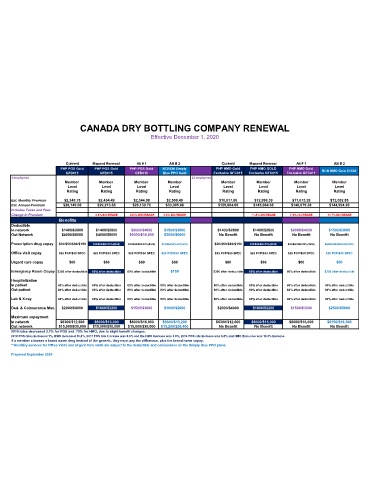
CANADA DRY BOTTLING COMPANY RENEWAL
Effective December 1, 2020
Current Mapped Renewal Alt # 1 Alt # 2 Current Mapped Renewal Alt # 1 Alt # 2
PHP POS Gold PHP POS Gold PHP POS Gold BCBSM Simply PHP HMO Gold PHP HMO GOLD PHP HMO Gold
GFD015 GFD015 GFD018 Blue PPO Gold Exclusive GFC015 Exclusive GFC015 Exclusive GFC011 BCN HMO Gold $1500
3 employees 22 employees
Member Member Member Member Member Member Member Member
Level Level Level Level Level Level Level Level
Rating Rating Rating Rating Rating Rating Rating Rating
Est. Monthly Premium $2,345.75 $2,434.49 $2,344.98 $2,500.49 $10,817.00 $12,090.39 $11,673.28 $12,082.85
Est. Annual Premium $28,149.00 $29,213.88 $28,139.76 $30,005.88 $129,804.00 $145,084.68 $140,079.36 $144,994.20
Includes Taxes and Fees
Change in Premium 3.8% INCREASE .033% DECREASE 6.6% INCREASE 11.8% INCREASE 7.9% INCREASE 11.7% INCREASE
Benefits
Deductible
In network $1400/$2800 $1400/$2800 $2000/$4000 $1500/$3000 $1400/$2800 $1400/$2800 $2000/$4000 $1500/$3000
Out Network $4000/$8000 $4000/$8000 $5000/$10,000 $3000/$6000 No Benefit No Benefit No Benefit No Benefit
Prescription drug copay $20/$50/$80/$150 $20/$50/$80/20%($300) $20/$50/$80/20%($300) $15/$50/50%/20%/25% $20/$50/$80/$150 $20/$50/$80/20%($300) $20/$50/$80/20%($300) $6/$25/$50/$80/20%/20%
Office visit copay $25 PCP/$50 SPEC $25 PCP/$50 SPEC $25 PCP/$50 SPEC $20 PCP/$40 SPEC $25 PCP/$50 SPEC $25 PCP/$50 SPEC $25 PCP/$50 SPEC $20 PCP/$40 SPEC
Urgent care copay $60 $60 $60 $60 $60 $60 $60 $50
Emergency Room Copay $300 after deductible 80% after deductible 80% after deductible $150 $300 after deductible 80% after deductible 80% after deductible $250 after deductible
Hospitalization
In patient 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible
Out patient 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible
Lab & X-ray 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible
Ded. & Coinsurance Max. $2000/$4000 $1600/$3200 $1500/$3000 $1000/$2000 $2000/$4000 $1600/$3200 $1500/$3000 $2500/$5000
Maximum copayment
In network $6300/$12,600 $8000/$16,000 $8000/$16,000 $6600/$13,200 $6300/$12,600 $8000/$16,000 $8000/$16,000 $8150/$16,300
Out network $15,000/$30,000 $15,000/$30,000 $15,000/$30,000 $13,200/$26,400 No Benefit No Benefit No Benefit No Benefit
2019 rates decreased 2.7% for POS and .75% for HMO, due to slight benefit changes.
2018 POS rates increased 1%, HMO increased 10.6%, 2017 POS rate increase was 8.6% and the HMO increase was 3.8%, 2016 POS rate increase was 8.8% and HMO Exclusive was 10.3% increase
If a member chooses a brand name drug instead of the generic, they must pay the difference, plus the brand name copay.
**Ancillary services for Office Visits and Urgent Care visits are subject to the deductible and coinsurance on the Simply Blue PPO plans.
Prepared September 2020