
Page 1721 - Cote clinical veterinary advisor dogs and cats 4th
P. 1721
866 Rectal Prolapse
osteotomy to access colorectal junction ○ Carcinoma in situ: median survival time • Careful surgical technique and strict asepsis
or cranial third of rectum • Guarded for malignant masses (p. 30) can decrease the risk of complications.
= 5-24 months; 55% recurrence rate
VetBooks.ir • Postoperatively, analgesia, stool softeners, and ○ Metastatic rate varies. Technician Tips
○ EEA stapling device transrectally
cool compresses for the first 2 days, followed
Monitor for depression, high fever, abdominal
○ Adenocarcinoma: mean survival time of 24
by warm compresses, should be used.
with electrocautery
tion, which may indicate infection or septic
• Antiinflammatory drugs therapeutically or months with cryosurgery, 18-29 months pain, vomiting, ileus, and perineal inflamma-
palliatively (e.g., piroxicam) ○ Radical surgery (e.g., rectal resections of peritonitis.
• Chemotherapy or radiation therapy more than 4 cm, colonic resection cranial
• Colostomy to the peritoneal reflection) can have a SUGGESTED READING
high complication rate and poor survival Baines SJ, et al: Rectum, anus, and perineum. In:
Possible Complications (<1 week). Johnston SA, et al, editors: Veterinary surgery—
• Postoperatively ○ Annular masses are poor prognostic small animal. ed 2, St. Louis, 2018, Elsevier, pp
○ Bleeding, mild tenesmus, stricture forma- indicators, with a median survival time 1783-1827.
tion, stenosis, rectal prolapse, perineal of 1.6 months. AUTHORS: Dena L. Lodato, DVM, MS, DACVS, CCRP;
hernia formation secondary to tenesmus, ○ Nodular or cobblestone masses have a Jennifer L. Wardlaw, DVM, MS, DACVS
perirectal abscesses, and recurrence median survival time of 12 months. EDITOR: Elizabeth A. Swanson, DVM, MS, DACVS
○ Septic peritonitis with colonic dehiscence ○ Single pedunculated masses that are
○ Fecal incontinence if pelvic plexus is completely excised can have a median
damaged, distal 1.5 cm of rectum is survival time of 32 months.
removed, or long rectal resection (>4 cm)
has been performed PEARLS & CONSIDERATIONS
○ Colostomy may result in skin excoriation.
Comments
PROGNOSIS & OUTCOME • Histopathology is required to determine
tumor type because cytology alone can result
• Good after resection of rectal polyps, in misdiagnosis.
carcinoma in situ, and leiomyomas • Endoscopy helps with assessment, but
○ Adenomatous polyps: median survival time biopsies obtained by this method may lead
= 2 years; 0%-41% recurrence rate to an incorrect diagnosis.
Rectal Prolapse Client Education
Sheet
BASIC INFORMATION HISTORY, CHIEF COMPLAINT
• Visualization of red tissue protruding from
Definition anus
Eversion of the anal mucosa or full-thickness • Straining to defecate (tenesmus) or urinate
rectal wall through the anal opening • Diarrhea
Epidemiology PHYSICAL EXAM FINDINGS
SPECIES, AGE, SEX • Partial prolapse: a few millimeters of red,
Can occur at any age, but young dogs and cats swollen mucosa protruding through anus
are most frequently affected. • Complete prolapse: cylindrical mass protrud-
ing from anus; tissue may be red, ulcerated,
GENETICS, BREED PREDISPOSITION or necrotic.
Manx cats may be predisposed. • Other findings consistent with underlying
cause for straining (e.g., enlarged prostate,
RISK FACTORS palpable neoplastic mass)
Recent perineal surgery, tenesmus
Etiology and Pathophysiology
ASSOCIATED DISORDERS • Animal affected by underlying disease that
Any condition that causes tenesmus may be causes straining
associated with rectal prolapse: gastrointestinal ○ In young/immature animals, intestinal
(GI) parasitism; neoplasia of the colon, rectum, parasites common
or anus; rectal foreign bodies; colitis; perineal • Repetitively increased intraabdominal
hernia; prostatic disease; urinary disease; dystocia pressure from straining causes weakness of
perirectal and perianal connective tissue or
Clinical Presentation muscles, resulting in prolapse.
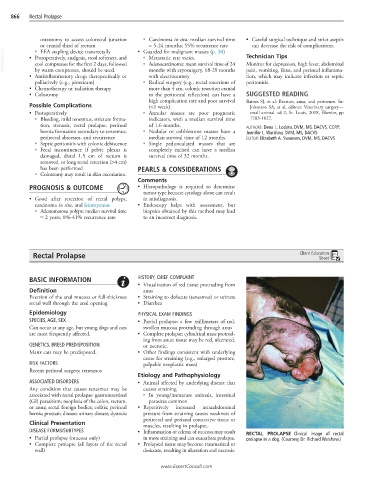
DISEASE FORMS/SUBTYPES • Inflammation or edema of mucosa may result RECTAL PROLAPSE Clinical image of rectal
• Partial prolapse (mucosa only) in more straining and can exacerbate prolapse. prolapse in a dog. (Courtesy Dr. Richard Walshaw.)
• Complete prolapse (all layers of the rectal • Prolapsed tissue may become traumatized or
wall) desiccate, resulting in ulceration and necrosis.
www.ExpertConsult.com