
Page 838 - Cote clinical veterinary advisor dogs and cats 4th
P. 838
Gunshot Wounds 401
VetBooks.ir Diseases and Disorders
A B C D
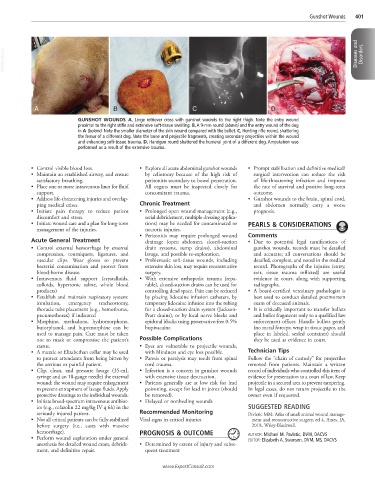
GUNSHOT WOUNDS A, Large retriever cross with gunshot wounds to the right thigh. Note the entry wound
proximal to the right stifle and extensive soft-tissue swelling. B, A 9-mm round (above) and the entry wound of the dog
in A (below). Note the smaller diameter of the skin wound compared with the bullet. C, Hunting rifle round, shattering
the femur of a different dog. Note the bone and projectile fragments, creating secondary projectiles within the wound
and enhancing soft-tissue trauma. D, Handgun round shattered the humeral joint of a different dog. Amputation was
performed as a result of the extensive trauma.
• Control visible blood loss. • Explore all acute abdominal gunshot wounds • Prompt stabilization and definitive medical/
• Maintain an established airway, and ensure by celiotomy because of the high risk of surgical intervention can reduce the risk
satisfactory breathing. peritonitis secondary to bowel penetration. of life-threatening infection and improve
• Place one or more intravenous lines for fluid All organs must be inspected closely for the rate of survival and positive long-term
support. concomitant trauma. outcome.
• Address life-threatening injuries and overlap- • Gunshot wounds to the brain, spinal cord,
ping medical crises. Chronic Treatment and abdomen normally carry a worse
• Initiate pain therapy to reduce patient • Prolonged open wound management (e.g., prognosis.
discomfort and stress. serial debridement, multiple dressing applica-
• Initiate wound care and a plan for long-term tions) may be needed for contaminated or PEARLS & CONSIDERATIONS
management of the injuries. necrotic injuries.
• Peritonitis may require prolonged wound Comments
Acute General Treatment drainage (open abdomen, closed-suction • Due to potential legal ramifications of
• Control external hemorrhage by external drain systems, sump drains), abdominal gunshot wounds, records must be detailed
compression, tourniquets, ligatures, and lavage, and possible re-exploration. and accurate; all conversations should be
vascular clips. Wear gloves to prevent • Problematic soft-tissue wounds, including detailed, complete, and noted in the medical
bacterial contamination and protect from extensive skin loss, may require reconstructive record. Photographs of the injuries (entry,
blood-borne disease. surgery. exit, tissue trauma inflicted) are useful
• Intravenous fluid support (crystalloids, • With extensive orthopedic trauma (repa- evidence in court, along with supporting
colloids, hypertonic saline, whole blood rable), closed-suction drains can be used for radiographs.
products) controlling dead space. Pain can be reduced • A board-certified veterinary pathologist is
• Establish and maintain respiratory system: by placing lidocaine infusion catheters, by best used to conduct detailed postmortem
intubation, emergency tracheostomy, temporary lidocaine infusion into the tubing exam of deceased animals.
thoracic tube placement (e.g., hemothorax, for a closed-suction drain system (Jackson- • It is critically important to transfer bullets
pneumothorax) if indicated Pratt drains), or by local nerve blocks and and bullet fragments only to a qualified law
• Morphine, methadone, hydromorphone, epidural blocks using preservative-free 0.5% enforcement officer. Handle bullets gently
butorphanol, and buprenorphine can be bupivacaine. (no metal forceps; wrap in tissue paper, and
used to manage pain. Care must be taken place in labeled, sealed container) should
not to mask or compromise the patient’s Possible Complications they be used as evidence in court.
status. • Eyes are vulnerable to projectile wounds,
• A muzzle or Elizabethan collar may be used with blindness and eye loss possible. Technician Tips
to protect attendants from being bitten by • Paresis or paralysis may result from spinal Follow the “chain of custody” for projectiles
the anxious or painful patient. cord trauma. removed from patients. Maintain a written
• Clip, clean, and pressure lavage (35-mL • Infection is a concern in gunshot wounds record of individuals who controlled this item of
syringe and an 18-gauge needle) the external with extensive tissue destruction. evidence for presentation to a court of law. Keep
wound; the wound may require enlargement • Patients generally are at low risk for lead projectile in a secured area to prevent tampering.
to prevent entrapment of lavage fluids. Apply poisoning, except for lead in joints (should In legal cases, do not return projectile to the
protective dressings to the individual wounds. be removed). owner even if requested.
• Initiate broad-spectrum intravenous antibiot- • Delayed or nonhealing wounds
ics (e.g., cefazolin 22 mg/kg IV q 6h) in the SUGGESTED READING
seriously injured patient. Recommended Monitoring Pavletic MM: Atlas of small animal wound manage-
• Not all critical patients can be fully stabilized Vital signs in critical injuries ment and reconstructive surgery, ed 4, Ames, IA,
before surgery (i.e., cases with massive 2018, Wiley-Blackwell.
hemorrhage). PROGNOSIS & OUTCOME
• Perform wound exploration under general AUTHOR: Michael M. Pavletic, DVM, DACVS
EDITOR: Elizabeth A. Swanson, DVM, MS, DACVS
anesthesia for detailed wound exam, debride- • Determined by extent of injury and subse-
ment, and definitive repair. quent treatment
www.ExpertConsult.com