
Page 128 - Clinical Pearls in Cardiology
P. 128
116 Clinical Pearls in Cardiology
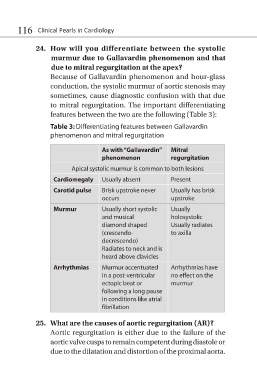
24. How will you differentiate between the systolic
murmur due to Gallavardin phenomenon and that
due to mitral regurgitation at the apex?
Because of Gallavardin phenomenon and hour-glass
conduction, the systolic murmur of aortic stenosis may
sometimes, cause diagnostic confusion with that due
to mitral regurgitation. The important differentiating
features between the two are the following (Table 3):
Table 3: Differentiating features between Gallavardin
phenomenon and mitral regurgitation
As with “Gallavardin” Mitral
phenomenon regurgitation
Apical systolic murmur is common to both lesions
Cardiomegaly Usually absent Present
Carotid pulse Brisk upstroke never Usually has brisk
occurs upstroke
Murmur Usually short systolic Usually
and musical holosystolic
diamond shaped Usually radiates
(crescendo- to axilla
decrescendo)
Radiates to neck and is
heard above clavicles
Arrhythmias Murmur accentuated Arrhythmias have
in a post-ventricular no effect on the
ectopic beat or murmur
following a long pause
in conditions like atrial
fibrillation
25. What are the causes of aortic regurgitation (AR)?
Aortic regurgitation is either due to the failure of the
aortic valve cusps to remain competent during diastole or
due to the dilatation and distortion of the proximal aorta.