
Page 40 - C:\Users\Andrew\Documents\Flip PDF Professional\Allstate Benefits Flip Book\
P. 40
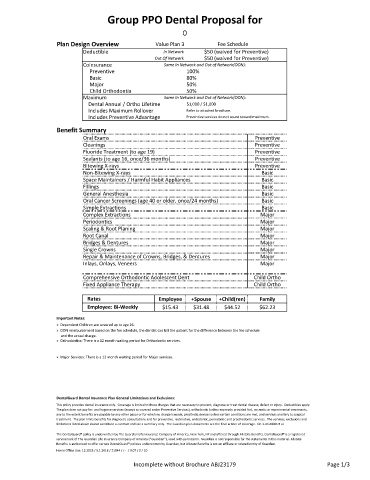
Group PPO Dental Proposal for
0
Plan Design Overview Value Plan 3 Fee Schedule
Deductible In Network $50 (waived for Preventive)
Out Of Network $50 (waived for Preventive)
Coinsurance Same In Network and Out of Network(OON):
Preventive 100%
Basic 80%
Major 50%
Child Orthodontia 50%
Maximum Same In Network and Out of Network(OON):
Dental Annual / Ortho Lifetime $1,000 / $1,000
Includes Maximum Rollover Refer to attached brochure.
Includes Preventive Advantage Preventive services do not count toward maximum.
Benefit Summary
Oral Exams Preventive
Cleanings Preventive
Fluoride Treatment (to age 19) Preventive
Sealants (to age 16, once/36 months) Preventive
Bitewing X‐rays Preventive
Non‐Bitewing X‐rays Basic
Space Maintainers / Harmful Habit Appliances Basic
Fillings Basic
General Anesthesia Basic
Oral Cancer Screenings (age 40 or older, once/24 months) Basic
Simple Extractions Basic
Complex Extractions Major
Periodontics Major
Scaling & Root Planing Major
Root Canal Major
Bridges & Dentures Major
Single Crowns Major
Repair & Maintenance of Crowns, Bridges, & Dentures Major
Inlays, Onlays, Veneers Major
Comprehensive Orthodontic Adolescent Dent Child Ortho
Fixed Appliance Therapy Child Ortho
Rates Employee +Spouse +Child(ren) Family
Employee: Bi‐Weekly $15.43 $31.48 $44.52 $62.23
Important Notes:
» Dependent Children are covered up to age 26.
» OON reimbursement based on the fee schedule, the dentist can bill the patient for the difference between the fee schedule
and the actual charge.
» Orthodontics: There is a 12 month waiting period for Orthodontic services.
» Major Services: There is a 12 month waiting period for Major services.
DentalGuard Dental Insurance Plan General Limitations and Exclusions:
This policy provides dental insurance only. Coverage is limited to those charges that are necessary to prevent, diagnose or treat dental disease, defect or injury. Deductibles apply.
The plan does not pay for: oral hygiene services (except as covered under Preventive Services), orthodontic (unless expressly provided for), cosmetic or experimental treatments,
any to the extent benefits are payable by any other payor or for which no charge is made, prosthetic devices unless certain conditions are met, and services ancillary to surgical
treatment. The plan limits benefits for diagnostic consultations and for preventive, restorative, endodontic, periodontic and prosthodontic services. The services, exclusions and
limitations listed above do not constitute a contract and are a summary only. The Guardian plan documents are the final arbiter of coverage. GP‐1‐DG2000 et al.
The DentalGuard® policy is underwritten by The Guardian Life Insurance Company of America, New York, NY and offered through Allstate Benefits. DentalGuard® is a registered
servicemark of The Guardian Life Insurance Company of America (''Guardian''), used with permission. Guardian is not responsible for the statements in this material. Allstate
Benefits is authorized to offer certain DentalGuard® policies underwritten by Guardian, but Allstate Benefits is not an affiliate or related entity of Guardian.
Home Office Use: 12.2018 / 9.1.2018 / 21044 / r ‐ / 0.07 / 0 / 10
Incomplete without Brochure ABJ23179 Page 1/3