
Page 251 - 2019 Orientation Manual
P. 251
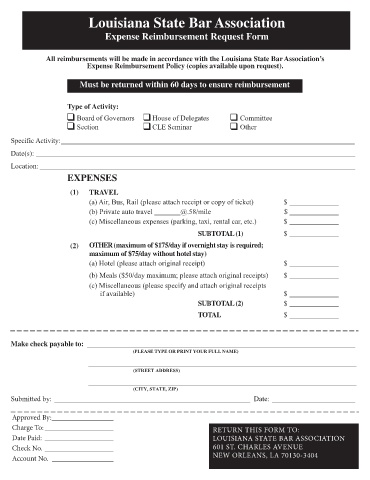
Louisiana State Bar Association
Expense Reimbursement Request Form
All reimbursements will be made in accordance with the Louisiana State Bar Association’s
Expense Reimbursement Policy (copies available upon request).
Must be returned within 60 days to ensure reimbursement
Type of Activity:
Board of Governors House of Delegates Committee
Section CLE Seminar Other
Specific Activity:
Date(s):
Location:
EXPENSES
(1) TRAVEL
(a) Air, Bus, Rail (please attach receipt or copy of ticket) $
(b) Private auto travel @.58/mile $
(c) Miscellaneous expenses (parking, taxi, rental car, etc.) $
SUBTOTAL (1) $
(2) OTHER (maximum of $175/day if overnight stay is required;
maximum of $75/day without hotel stay)
(a) Hotel (please attach original receipt) $
(b) Meals ($50/day maximum; please attach original receipts) $
(c) Miscellaneous (please specify and attach original receipts
if available) $
SUBTOTAL (2) $
TOTAL $
Make check payable to:
(PLEASE TYPE OR PRINT YOUR FULL NAME)
(STREET ADDRESS)
(CITY, STATE, ZIP)
Submitted by: Date:
Approved By:
Charge To: RETURN THIS FORM TO:
Date Paid: LOUISIANA STATE BAR ASSO CIATION
Check No. 601 ST. CHARLES AVENUE
Account No. NEW ORLEANS, LA 70130-3404