
Page 9 - QSC Benefits Guide 7-17 SLO
P. 9
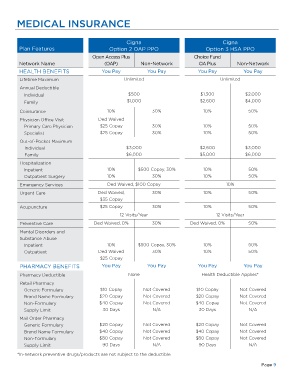
MEDICAL INSURANCE
Cigna Cigna
Plan Features Option 2 OAP PPO Option 3 HSA PPO
Open Access Plus Choice Fund
Network Name (OAP) Non-Network OA Plus Non-Network
HEALTH BENEFITS You Pay You Pay You Pay You Pay
Lifetime Maximum Unlimited Unlimited
Annual Deductible
Individual $500 $1,300 $2,000
Family $1,000 $2,600 $4,000
Coinsurance 10% 30% 10% 50%
Physician Office Visit Ded Waived
Primary Care Physician $25 Copay 30% 10% 50%
Specialist $25 Copay 30% 10% 50%
Out-of-Pocket Maximum
Individual $3,000 $2,600 $3,000
Family $6,000 $5,000 $6,000
Hospitalization
Inpatient 10% $500 Copay, 30% 10% 50%
Outpatient Surgery 10% 30% 10% 50%
Emergency Services Ded Waived, $100 Copay 10%
Urgent Care Ded Waived, 30% 10% 50%
$35 Copay
Acupuncture $25 Copay 30% 10% 50%
12 Visits/Year 12 Visits/Year
Preventive Care Ded Waived, 0% 30% Ded Waived, 0% 50%
Mental Disorders and
Substance Abuse
Inpatient 10% $500 Copay, 30% 10% 50%
Outpatient Ded Waived 30% 10% 50%
$25 Copay
PHARMACY BENEFITS You Pay You Pay You Pay You Pay
Pharmacy Deductible None Health Deductible Applies*
Retail Pharmacy
Generic Formulary $10 Copay Not Covered $10 Copay Not Covered
Brand Name Formulary $20 Copay Not Covered $20 Copay Not Covered
Non-Formulary $40 Copay Not Covered $40 Copay Not Covered
Supply Limit 30 Days N/A 30 Days N/A
Mail Order Pharmacy
Generic Formulary $20 Copay Not Covered $20 Copay Not Covered
Brand Name Formulary $40 Copay Not Covered $40 Copay Not Covered
Non-Formulary $80 Copay Not Covered $80 Copay Not Covered
Supply Limit 90 Days N/A 90 Days N/A
*In-network preventive drugs/products are not subject to the deductible.
Page 9