
Page 11 - Incipio EE Guide 01-19 Non-CA Bi-Weekly
P. 11
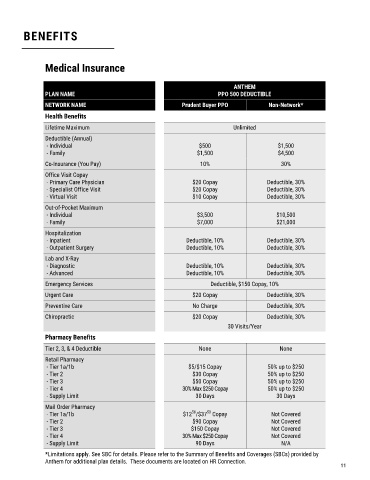
BENEFITS
Medical Insurance
ANTHEM
PLAN NAME PPO 500 DEDUCTIBLE
NETWORK NAME Prudent Buyer PPO Non-Network*
Health Benefits
Lifetime Maximum Unlimited
Deductible (Annual)
- Individual $500 $1,500
- Family $1,500 $4,500
Co-Insurance (You Pay) 10% 30%
Office Visit Copay
- Primary Care Physician $20 Copay Deductible, 30%
- Specialist Office Visit $20 Copay Deductible, 30%
- Virtual Visit $10 Copay Deductible, 30%
Out-of-Pocket Maximum
- Individual $3,500 $10,500
- Family $7,000 $21,000
Hospitalization
- Inpatient Deductible, 10% Deductible, 30%
- Outpatient Surgery Deductible, 10% Deductible, 30%
Lab and X-Ray
- Diagnostic Deductible, 10% Deductible, 30%
- Advanced Deductible, 10% Deductible, 30%
Emergency Services Deductible, $150 Copay, 10%
Urgent Care $20 Copay Deductible, 30%
Preventive Care No Charge Deductible, 30%
Chiropractic $20 Copay Deductible, 30%
30 Visits/Year
Pharmacy Benefits
Tier 2, 3, & 4 Deductible None None
Retail Pharmacy
- Tier 1a/1b $5/$15 Copay 50% up to $250
- Tier 2 $30 Copay 50% up to $250
- Tier 3 $50 Copay 50% up to $250
- Tier 4 30% Max $250 Copay 50% up to $250
- Supply Limit 30 Days 30 Days
Mail Order Pharmacy
50
50
- Tier 1a/1b $12 /$37 Copay Not Covered
- Tier 2 $90 Copay Not Covered
- Tier 3 $150 Copay Not Covered
- Tier 4 30% Max $250 Copay Not Covered
- Supply Limit 90 Days N/A
*Limitations apply. See SBC for details. Please refer to the Summary of Benefits and Coverages (SBCs) provided by
Anthem for additional plan details. These documents are located on HR Connection.
11