
Page 3 - Example-Lucas Museum Recruiting Guide_082019
P. 3
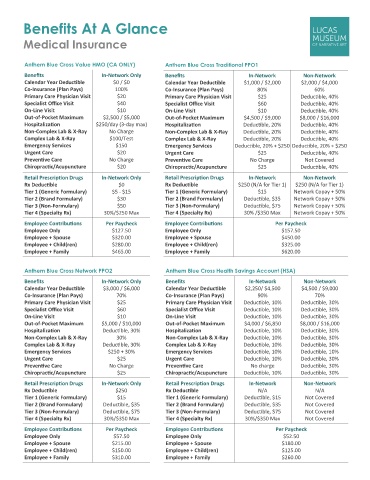
Benefits At A Glance
Medical Insurance
Anthem Blue Cross Value HMO (CA ONLY) Anthem Blue Cross Traditional PPO1
Benefits In-Network Only Benefits In-Network Non-Network
Calendar Year Deductible $0 / $0 Calendar Year Deductible $1,000 / $2,000 $2,000 / $4,000
Co-Insurance (Plan Pays) 100% Co-Insurance (Plan Pays) 80% 60%
Primary Care Physician Visit $20 Primary Care Physician Visit $25 Deductible, 40%
Specialist Office Visit $40 Specialist Office Visit $60 Deductible, 40%
On-Line Visit $10 On-Line Visit $10 Deductible, 40%
Out-of-Pocket Maximum $2,500 / $5,000 Out-of-Pocket Maximum $4,500 / $9,000 $8,000 / $16,000
Hospitalization $250/day (3-day max) Hospitalization Deductible, 20% Deductible, 40%
Non-Complex Lab & X-Ray No Charge Non-Complex Lab & X-Ray Deductible, 20% Deductible, 40%
Complex Lab & X-Ray $100/Test Complex Lab & X-Ray Deductible, 20% Deductible, 40%
Emergency Services $150 Emergency Services Deductible, 20% + $250 Deductible, 20% + $250
Urgent Care $20 Urgent Care $25 Deductible, 40%
Preventive Care No Charge Preventive Care No Charge Not Covered
Chiropractic/Acupuncture $20 Chiropractic/Acupuncture $25 Deductible, 40%
Retail Prescription Drugs In-Network Only Retail Prescription Drugs In-Network Non-Network
Rx Deductible $0 Rx Deductible $250 (N/A for Tier 1) $250 (N/A for Tier 1)
Tier 1 (Generic Formulary) $5 - $15 Tier 1 (Generic Formulary) $15 Network Copay + 50%
Tier 2 (Brand Formulary) $30 Tier 2 (Brand Formulary) Deductible, $35 Network Copay + 50%
Tier 3 (Non-Formulary) $50 Tier 3 (Non-Formulary) Deductible, $75 Network Copay + 50%
Tier 4 (Specialty Rx) 30%/$250 Max Tier 4 (Specialty Rx) 30% /$350 Max Network Copay + 50%
Employee Contributions Per Paycheck Employee Contributions Per Paycheck
Employee Only $127.50 Employee Only $157.50
Employee + Spouse $320.00 Employee + Spouse $450.00
Employee + Child(ren) $280.00 Employee + Child(ren) $325.00
Employee + Family $465.00 Employee + Family $620.00
Anthem Blue Cross Network PPO2 Anthem Blue Cross Health Savings Account (HSA)
Benefits In-Network Only Benefits In-Network Non-Network
Calendar Year Deductible $3,000 / $6,000 Calendar Year Deductible $2,250/ $4,500 $4,500 / $9,000
Co-Insurance (Plan Pays) 70% Co-Insurance (Plan Pays) 90% 70%
Primary Care Physician Visit $25 Primary Care Physician Visit Deductible, 10% Deductible, 30%
Specialist Office Visit $60 Specialist Office Visit Deductible, 10% Deductible, 30%
On-Line Visit $10 On-Line Visit Deductible, 10% Deductible, 30%
Out-of-Pocket Maximum $5,000 / $10,000 Out-of-Pocket Maximum $4,000 / $6,850 $8,000 / $16,000
Hospitalization Deductible, 30% Hospitalization Deductible, 10% Deductible, 30%
Non-Complex Lab & X-Ray 30% Non-Complex Lab & X-Ray Deductible, 10% Deductible, 30%
Complex Lab & X-Ray Deductible, 30% Complex Lab & X-Ray Deductible, 10% Deductible, 30%
Emergency Services $250 + 30% Emergency Services Deductible, 10% Deductible, 10%
Urgent Care $25 Urgent Care Deductible, 10% Deductible, 30%
Preventive Care No Charge Preventive Care No charge Deductible, 30%
Chiropractic/Acupuncture $25 Chiropractic/Acupuncture Deductible, 10% Deductible, 30%
Retail Prescription Drugs In-Network Only Retail Prescription Drugs In-Network Non-Network
Rx Deductible $250 Rx Deductible N/A N/A
Tier 1 (Generic Formulary) $15 Tier 1 (Generic Formulary) Deductible, $15 Not Covered
Tier 2 (Brand Formulary) Deductible, $35 Tier 2 (Brand Formulary) Deductible, $35 Not Covered
Tier 3 (Non-Formulary) Deductible, $75 Tier 3 (Non-Formulary) Deductible, $75 Not Covered
Tier 4 (Specialty Rx) 30%/$350 Max Tier 4 (Specialty Rx) 30%/$350 Max Not Covered
Employee Contributions Per Paycheck Employee Contributions Per Paycheck
Employee Only $57.50 Employee Only $52.50
Employee + Spouse $215.00 Employee + Spouse $180.00
Employee + Child(ren) $150.00 Employee + Child(ren) $125.00
Employee + Family $310.00 Employee + Family $260.00