
Page 10 - Volcom Benefit Summary 2019 CA
P. 10
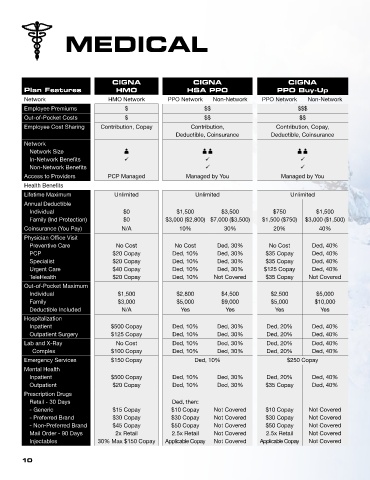
MEDICAL
CIGNA CIGNA CIGNA
Plan Features HMO HSA PPO PPO Buy-Up
Network HMO Network PPO Network Non-Network PPO Network Non-Network
Employee Premiums $ $$ $$$
Out-of-Pocket Costs $ $$ $$
Employee Cost Sharing Contribution, Copay Contribution, Contribution, Copay,
Deductible, Coinsurance Deductible, Coinsurance
Network
Network Size A AA AA
In-Network Benefits ü ü ü
Non-Network Benefits ü ü
Access to Providers PCP Managed Managed by You Managed by You
Health Benefits
Lifetime Maximum Unlimited Unlimited Unlimited
Annual Deductible
Individual $0 $1,500 $3,500 $750 $1,500
Family (Ind Protection) $0 $3,000 ($2,800) $7,000 ($3,500) $1,500 ($750) $3,000 ($1,500)
Coinsurance (You Pay) N/A 10% 30% 20% 40%
Physician Office Visit
Preventive Care No Cost No Cost Ded, 30% No Cost Ded, 40%
PCP $20 Copay Ded, 10% Ded, 30% $35 Copay Ded, 40%
Specialist $20 Copay Ded, 10% Ded, 30% $35 Copay Ded, 40%
Urgent Care $40 Copay Ded, 10% Ded, 30% $125 Copay Ded, 40%
TeleHealth $20 Copay Ded, 10% Not Covered $35 Copay Not Covered
Out-of-Pocket Maximum
Individual $1,500 $2,800 $4,500 $2,500 $5,000
Family $3,000 $5,000 $9,000 $5,000 $10,000
Deductible Included N/A Yes Yes Yes Yes
Hospitalization
Inpatient $500 Copay Ded, 10% Ded, 30% Ded, 20% Ded, 40%
Outpatient Surgery $125 Copay Ded, 10% Ded, 30% Ded, 20% Ded, 40%
Lab and X-Ray No Cost Ded, 10% Ded, 30% Ded, 20% Ded, 40%
Complex $100 Copay Ded, 10% Ded, 30% Ded, 20% Ded, 40%
Emergency Services $150 Copay Ded, 10% $250 Copay
Mental Health
Inpatient $500 Copay Ded, 10% Ded, 30% Ded, 20% Ded, 40%
Outpatient $20 Copay Ded, 10% Ded, 30% $35 Copay Ded, 40%
Prescription Drugs
Retail - 30 Days Ded, then:
- Generic $15 Copay $10 Copay Not Covered $10 Copay Not Covered
- Preferred Brand $30 Copay $30 Copay Not Covered $30 Copay Not Covered
- Non-Preferred Brand $45 Copay $50 Copay Not Covered $50 Copay Not Covered
Mail Order - 90 Days 2x Retail 2.5x Retail Not Covered 2.5x Retail Not Covered
Injectables 30% Max $150 Copay Applicable Copay Not Covered Applicable Copay Not Covered
10