
Page 101 - New Hire Kit (Non-Union)
P. 101
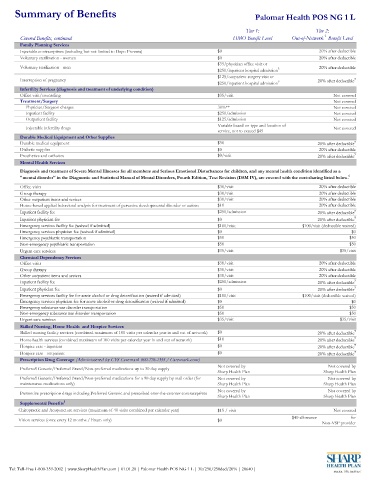
Summary of Benefits Palomar Health POS NG 1 L
Tier 1: Tier 2:
1
Covered Benefits, continued HMO Benefit Level Out-of-Network Benefit Level
Family Planning Services
Injectable contraceptives (including but not limited to Depo Provera) $0 20% after deductible
Voluntary sterilization - women $0 20% after deductible
$35/physician office visit or
Voluntary sterilization - men 5 20% after deductible
$250/inpatient hospital admission
$125/outpatient surgery visit or
Interruption of pregnancy 5 20% after deductible 7
$250/inpatient hospital admission
Infertility Services (diagnosis and treatment of underlying condition)
Office visit/counseling $35/visit Not covered
Treatment/Surgery Not covered
Physician/Surgeon charges 30%** Not covered
Inpatient facility $250/admission Not covered
Outpatient facility $125/admission Not covered
Variable based on type and location of
Injectable infertility drugs Not covered
service, not to exceed $45
Durable Medical Equipment and Other Supplies
Durable medical equipment $50 20% after deductible 7
Diabetic supplies $0 20% after deductible
Prosthetics and orthotics $0/visit 20% after deductible 7
Mental Health Services
Diagnosis and treatment of Severe Mental Illnesses for all members and Serious Emotional Disturbances for children, and any mental health condition identified as a
"mental disorder" in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM IV), are covered with the cost-sharing listed below. 6
Office visits $30/visit 20% after deductible
Group therapy $30/visit 20% after deductible
Other outpatient items and sevices $30/visit 20% after deductible
Home-based applied behavioral analysis for treatment of pervasive developmental disorder or autism $10 20% after deductible
Inpatient facility fee $250/admission 20% after deductible 7
Inpatient physician fee $0 20% after deductible 7
Emergency services facility fee (waived if admitted) $100/visit $100/visit (deductible waived)
Emergency services physician fee (waived if admitted) $0 $0
Emergency psychiatric transportation $50 $50
Non-emergency psychiatric transportation $50 $50
Urgent care services $35/visit $35/visit
Chemical Dependency Services
Office visits $30/visit 20% after deductible
Group therapy $30/visit 20% after deductible
Other outpatient items and sevices $30/visit 20% after deductible
Inpatient facility fee $250/admission 20% after deductible 7
Inpatient physician fee $0 20% after deductible 7
Emergency services facility fee for acute alcohol or drug detoxification (waived if admitted) $100/visit $100/visit (deductible waived)
Emergency services physician fee for acute alcohol or drug detoxification (waived if admitted) $0 $0
Emergency substance use disorder transportation $50 $50
Non-emergency substance use disorder transportation $50 $50
Urgent care services $35/visit $35/visit
Skilled Nursing, Home Health and Hospice Services
Skilled nursing facility services (combined maximum of 100 visits per calendar year in and out of network) $0 20% after deductible 7
Home health services (combined maximum of 100 visits per calendar year in and out of network) $10 20% after deductible 7
Hospice care - inpatient $0 20% after deductible 7
Hospice care - outpatient $0 20% after deductible 7
Prescription Drug Coverage (Administered by CVS Caremark 800-776-1355 / Caremark.com)
Not covered by Not covered by
Preferred Generic/Preferred Brand/Non-preferred medications up to 30 day supply
Sharp Health Plan Sharp Health Plan
Preferred Generic/Preferred Brand/Non-preferred medications for a 90 day supply by mail order (for Not covered by Not covered by
maintenance medications only) Sharp Health Plan Sharp Health Plan
Not covered by Not covered by
Preventive prescription drugs including Preferred Generic and prescribed over-the-counter contraceptives
Sharp Health Plan Sharp Health Plan
Supplemental Benefits 1
Chiropractic and Acupuncture services (maximum of 40 visits combined per calendar year) $15 / visit Not covered
$40 allowance for
Vision services (once every 12 months / Exam only) $0
Non-VSP provider
Tel: Toll-Free 1-800-359-2002 | www.SharpHealthPlan.com | 01.01.20 | Palomar Health POS NG 1 L | 30/250/250ded/20% | 20640 |