
Page 11 - Burnham BG 2018-19 v4
P. 11
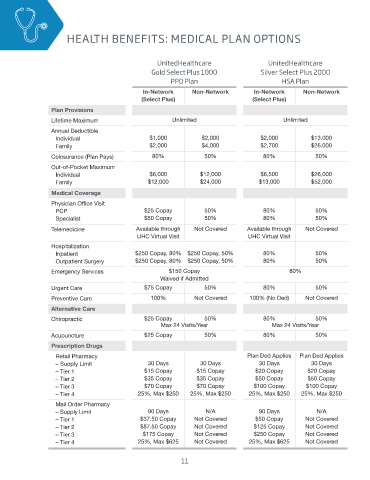
HEALTH BENEFITS: MEDICAL PLAN OPTIONS HEALTH BENEFITS: MEDICAL PLAN OPTIONS
UnitedHealthcare UnitedHealthcare
Gold Select Plus 1000 Silver Select Plus 2000
PPO Plan HSA Plan
In-Network Non-Network In-Network Non-Network
(Select Plus) (Select Plus)
Plan Provisions
Lifetime Maximum Unlimited Unlimited
Annual Deductible
Individual $1,000 $2,000 $2,000 $13,000
Family $2,000 $4,000 $2,700 $26,000
Coinsurance (Plan Pays) 80% 50% 80% 50%
Out-of-Pocket Maximum
Individual $6,000 $12,000 $6,500 $26,000
Family $12,000 $24,000 $13,000 $52,000
Medical Coverage
Physician Office Visit
PCP $25 Copay 50% 80% 50%
Specialist $50 Copay 50% 80% 50%
Telemedicine Available through Not Covered Available through Not Covered
UHC Virtual Visit UHC Virtual Visit
Hospitalization
Inpatient $250 Copay, 80% $250 Copay, 50% 80% 50%
Outpatient Surgery $250 Copay, 80% $250 Copay, 50% 80% 50%
Emergency Services $150 Copay 80%
Waived if Admitted
Urgent Care $75 Copay 50% 80% 50%
Preventive Care 100% Not Covered 100% (No Ded) Not Covered
Alternative Care
Chiropractic $25 Copay 50% 80% 50%
Max 24 Visits/Year Max 24 Visits/Year
Acupuncture $25 Copay 50% 80% 50%
Prescription Drugs
Retail Pharmacy Plan Ded Applies Plan Ded Applies
– Supply Limit 30 Days 30 Days 30 Days 30 Days
– Tier 1 $15 Copay $15 Copay $20 Copay $20 Copay
– Tier 2 $35 Copay $35 Copay $50 Copay $50 Copay
– Tier 3 $70 Copay $70 Copay $100 Copay $100 Copay
– Tier 4 25%, Max $250 25%, Max $250 25%, Max $250 25%, Max $250
Mail Order Pharmacy
– Supply Limit 90 Days N/A 90 Days N/A
– Tier 1 $37.50 Copay Not Covered $50 Copay Not Covered
– Tier 2 $87.50 Copay Not Covered $125 Copay Not Covered
– Tier 3 $175 Copay Not Covered $250 Copay Not Covered
– Tier 4 25%, Max $625 Not Covered 25%, Max $625 Not Covered
11