
Page 8 - Ria Benefits Guide 2020 FINAL CO
P. 8
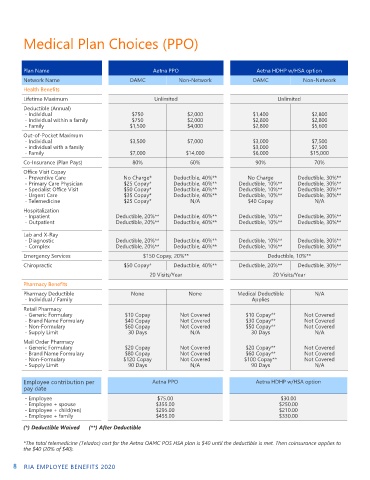
Medical Plan Choices (PPO)
Plan Name MEDICAL Aetna PPO Aetna HDHP w/HSA option
Network Name OAMC Non-Network OAMC Non-Network
Health Benefits
Lifetime Maximum Unlimited Unlimited
Deductible (Annual)
- Individual $750 $2,000 $1,400 $2,800
- Individual within a family $750 $2,000 $2,800 $2,800
- Family $1,500 $4,000 $2,800 $5,600
Out-of-Pocket Maximum
- Individual $3,500 $7,000 $3,000 $7,500
- individual with a family $3,000 $7,500
- Family $7,000 $14,000 $6,000 $15,000
Co-Insurance (Plan Pays) 80% 60% 90% 70%
Office Visit Copay
- Preventive Care No Charge* Deductible, 40%** No Charge Deductible, 30%**
- Primary Care Physician $25 Copay* Deductible, 40%** Deductible, 10%** Deductible, 30%**
- Specialist Office Visit $50 Copay* Deductible, 40%** Deductible, 10%** Deductible, 30%**
- Urgent Care $35 Copay* Deductible, 40%** Deductible, 10%** Deductible, 30%**
- Telemedicine $25 Copay* N/A $40 Copay N/A
Hospitalization
- Inpatient Deductible, 20%** Deductible, 40%** Deductible, 10%** Deductible, 30%**
- Outpatient Deductible, 20%** Deductible, 40%** Deductible, 10%** Deductible, 30%**
Lab and X-Ray
- Diagnostic Deductible, 20%** Deductible, 40%** Deductible, 10%** Deductible, 30%**
- Complex Deductible, 20%** Deductible, 40%** Deductible, 10%** Deductible, 30%**
Emergency Services $150 Copay, 20%** Deductible, 10%**
Chiropractic $50 Copay* Deductible, 40%** Deductible, 20%** Deductible, 30%**
20 Visits/Year 20 Visits/Year
Pharmacy Benefits
Pharmacy Deductible None None Medical Deductible N/A
- Individual / Family Applies
Retail Pharmacy
- Generic Formulary $10 Copay Not Covered $10 Copay** Not Covered
- Brand Name Formulary $40 Copay Not Covered $30 Copay** Not Covered
- Non-Formulary $60 Copay Not Covered $50 Copay** Not Covered
- Supply Limit 30 Days N/A 30 Days N/A
Mail Order Pharmacy
- Generic Formulary $20 Copay Not Covered $20 Copay** Not Covered
- Brand Name Formulary $80 Copay Not Covered $60 Copay** Not Covered
- Non-Formulary $120 Copay Not Covered $100 Copay** Not Covered
- Supply Limit 90 Days N/A 90 Days N/A
Employee contribution per Aetna PPO Aetna HDHP w/HSA option
pay date
- Employee $75.00 $30.00
- Employee + spouse $355.00 $250.00
- Employee + child(ren) $295.00 $210.00
- Employee + family $455.00 $330.00
(*) Deductible Waived (**) After Deductible
*The total telemedicine (Teladoc) cost for the Aetna OAMC POS HSA plan is $40 until the deductible is met. Then coinsurance applies to
the $40 (20% of $40).
8 RIA EMPLOYEE BENEFITS 2020