
Page 62 - New Hire Kit (Union)
P. 62
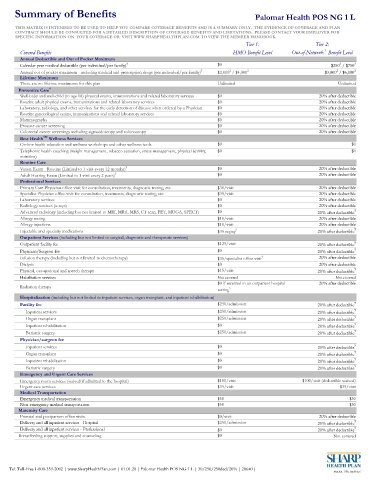
Summary of Benefits Palomar Health POS NG 1 L
THIS MATRIX IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE EVIDENCE OF COVERAGE AND PLAN
CONTRACT SHOULD BE CONSULTED FOR A DETAILED DESCRIPTION OF COVERAGE BENEFITS AND LIMITATIONS. PLEASE CONTACT YOUR EMPLOYER FOR
SPECIFIC INFORMATION ON YOUR COVERAGE OR VISIT WWW.SHARPHEALTHPLAN.COM TO VIEW THE MEMBER HANDBOOK.
Tier 1: Tier 2:
1
Covered Benefits HMO Benefit Level Out-of-Network Benefit Level
Annual Deductible and Out of Pocket Maximum
2
Calendar year medical deductible (per individual/per family) 3 $0 $250 / $750 2
2
2
Annual out of pocket maximum - including medical and prescription drugs (per individual/per family) 3 $2,000 / $4,000 2 $3,000 / $6,000 2
Lifetime Maximum
There are no lifetime maximums for this plan Unlimited Unlimited
Preventive Care 4
Well-baby and well-child (to age 18) physical exams, immunizations and related laboratory services $0 20% after deductible
Routine adult physical exams, immunizations and related laboratory services $0 20% after deductible
Laboratory, radiology, and other services for the early detection of disease when ordered by a Physician $0 20% after deductible
Routine gynecological exams, immunizations and related laboratory services $0 20% after deductible
Mammography $0 20% after deductible
Prostate cancer screening $0 20% after deductible
Colorectal cancer screenings including sigmoidoscopy and colonoscopy $0 20% after deductible
SM
Best Health Wellness Services
On-line health education and wellness workshops and other wellness tools $0 $0
Telephonic health coaching (weight management, tobacco cessation, stress management, physical activity, $0 $0
nutrition)
Routine Care
Vision Exam - Routine (Limited to 1 visit every 12 months) 3 $0 20% after deductible
Adult Hearing Exam (Limited to 1 visit every 2 years) 3 $0 20% after deductible
Professional Services
Primary Care Physician office visit for consultation, treatments, diagnostic testing, etc. $30/visit 20% after deductible
Specialist Physician office visit for consultation, treatments, diagnostic testing, etc. $35/visit 20% after deductible
Laboratory services $0 20% after deductible
Radiology services (x-rays) $0 20% after deductible
Advanced radiology (including but not limited to MRI, MRA, MRS, CT scan, PET, MUGA, SPECT) $0 20% after deductible 7
Allergy testing $10/visit 20% after deductible
Allergy injections $10/visit 20% after deductible
Injectable and specialty medications $35 copay 5 20% after deductible 7
Outpatient Services (including but not limited to surgical, diagnostic and therapeutic services)
Outpatient facility fee $125/visit 20% after deductible 7
Physician/Surgeon fee $0 20% after deductible 7
Infusion therapy (including but not limited to chemotherapy) $35/specialist office visit 5 20% after deductible
Dialysis $0 20% after deductible
Physical, occupational and speech therapy $15/visit 20% after deductible 7
Habilitation services Not covered Not covered
$0 if received in an outpatient hospital 20% after deductible
Radiation therapy 5
setting
Hospitalization (including but not limited to inpatient services, organ transplant, and inpatient rehabilitation)
Facility fee $250/admission 20% after deductible 7
Inpatient services $250/admission 20% after deductible 7
Organ transplant $250/admission 20% after deductible 7
Inpatient rehabilitation $0 20% after deductible 7
Bariatric surgery $250/admission 20% after deductible 7
Physician/surgeon fee
Inpatient services $0 20% after deductible 7
Organ transplant $0 20% after deductible 7
Inpatient rehabilitation $0 20% after deductible 7
Bariatric surgery $0 20% after deductible 7
Emergency and Urgent Care Services
Emergency room services (waived if admitted to the hospital) $100/visit $100/visit (deductible waived)
Urgent care services $35/visit $35/visit
Medical Transportation
Emergency medical transportation $50 $50
Non-emergency medical transportation $50 $50
Maternity Care
Prenatal and postpartum office visits $0/visit 20% after deductible
Delivery and all inpatient services - Hospital $250/admission 20% after deductible 7
Delivery and all inpatient services - Professional $0 20% after deductible 7
Breastfeeding support, supplies and counseling $0 Not covered
Tel: Toll-Free 1-800-359-2002 | www.SharpHealthPlan.com | 01.01.20 | Palomar Health POS NG 1 L | 30/250/250ded/20% | 20640 |