
Page 76 - New Hire Kit (Union)
P. 76
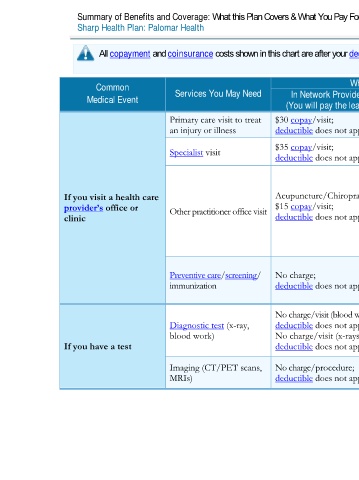
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2020 – 12/31/2020
Sharp Health Plan: Palomar Health Coverage for: Individual / Family | Plan Type: POS
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common What You Will Pay Limitations, Exceptions, & Other
Medical Event Services You May Need In Network Provider Out-of-Network Provider Important Information
(You will pay the least) (You will pay the most)
Primary care visit to treat $30 copay/visit; 20% coinsurance None
an injury or illness deductible does not apply
$35 copay/visit; Preauthorization is required, except for
Specialist visit 20% coinsurance
deductible does not apply obstetric gynecologic services.
Acupuncture/Chiropractic coverage is
limited to 40 combined visits/calendar year
If you visit a health care Acupuncture/Chiropractic: without preauthorization.
provider’s office or Other practitioner office visit $15 copay/visit; Not covered
clinic deductible does not apply Cost sharing for covered supplemental
Acupuncture/Chiropractic services do not
count towards the out–of–pocket limit.
You may have to pay for services that aren’t
Preventive care/screening/ No charge; 20% coinsurance preventive. Ask your provider if the services
immunization deductible does not apply you need are preventive. Then check what
your plan will pay for.
No charge/visit (blood work);
Diagnostic test (x-ray, deductible does not apply 20% coinsurance (blood work) None
blood work) No charge/visit (x-rays); 20% coinsurance (x-rays)
If you have a test deductible does not apply
Imaging (CT/PET scans, No charge/procedure; Preauthorization is required.
MRIs) deductible does not apply 20% coinsurance Precertification applies Out-of-Network.
2 of 11
Palomar Health POS NG 1 L / ACCH15_40 / VSA0