
Page 7 - Oremor Benefits Flipbook
P. 7
Benefits
Medical Insurance
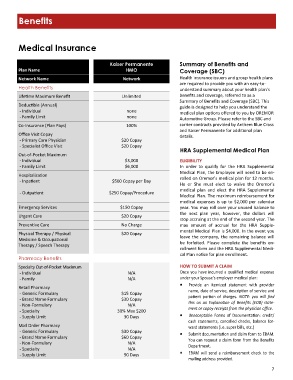
Kaiser Permanente Summary of Benefits and
Plan Name HMO Coverage (SBC)
Network Name Network Health insurance issuers and group health plans
are required to provide you with an easy-to-
Health Benefits understand summary about your health plan’s
Lifetime Maximum Benefit Unlimited benefits and coverage, referred to as a
Summary of Benefits and Coverage (SBC). This
Deductible (Annual)
guide is designed to help you understand the
- Individual none
medical plan options offered to you by OREMOR
- Family Limit none
Automotive Group. Please refer to the SBC and
Co-Insurance (Plan Pays) 100% carrier contracts provided by Anthem Blue Cross
and Kaiser Permanente for additional plan
Office Visit Copay
details.
- Primary Care Physician $20 Copay
- Specialist Office Visit $20 Copay
HRA Supplemental Medical Plan
Out-of-Pocket Maximum
- Individual $3,000 ELIGIBILITY
- Family Limit $6,000 In order to qualify for the HRA Supplemental
Medical Plan, the Employee will need to be en‐
Hospitalization rolled on Oremor’s medical plan for 12 months.
- Inpatient $500 Copay per Day He or She must elect to waive the Oremor’s
- Outpatient $250 Copay/Procedure medical plan and elect the HRA Supplemental
Medical Plan. The maximum reimbursement for
medical expenses is up to $2,000 per calendar
Emergency Services $150 Copay year. You may roll over your unused balance to
the next plan year, however, the dollars will
Urgent Care $20 Copay
stop accruing at the end of the second year. The
Preventive Care No Charge max amount of accrual for the HRA Supple‐
mental Medical Plan is $4,000. In the event you
Physical Therapy / Physical $20 Copay leave the company, the remaining balance will
Medicine & Occupational
be forfeited. Please complete the benefits en‐
Therapy / Speech Therapy
rollment form and the HRA Supplemental Medi‐
cal Plan notice for plan enrollment.
Pharmacy Benefits
Specialty Out-of-Pocket Maximum HOW TO SUBMIT A CLAIM
- Individual N/A Once you have incurred a qualified medical expense
- Family N/A under your Spouse’s employer medical plan:
Provide an itemized statement with provider
Retail Pharmacy
name, date of service, description of service and
- Generic Formulary $15 Copay
- Brand Name Formulary $30 Copay patient portion of charges. NOTE: you will find
- Non-Formulary N/A this on an Explanation of Benefits (EOB) state-
ment or copay receipts from the physician office.
- Specialty 30% Max $200
- Supply Limit 30 Days Unacceptable Forms of Documentation: credit/
cash statements, cancelled checks, balance for‐
Mail Order Pharmacy ward statements (i.e. super bills, etc.)
- Generic Formulary $30 Copay Submit documentation and claim form to EBAM.
- Brand Name Formulary $60 Copay You can request a claim form from the Benefits
- Non-Formulary N/A
Department.
- Specialty N/A
- Supply Limit 90 Days EBAM will send a reimbursement check to the
mailing address provided.
7