
Page 6 - Confie Retail Benefits Guide 01-18_FINAL_r2_dp wording
P. 6
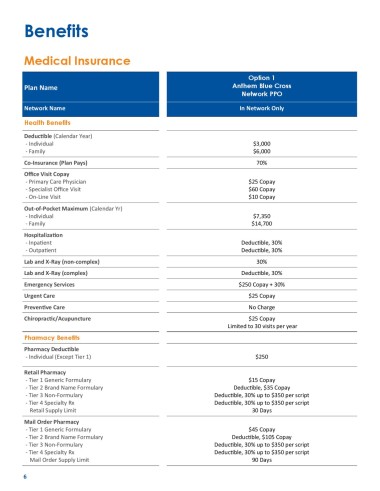
Benefits
Medical Insurance
Option 1
Plan Name Anthem Blue Cross
Network PPO
Network Name In Network Only
Health Benefits
Deductible (Calendar Year)
- Individual $3,000
- Family $6,000
Co-Insurance (Plan Pays) 70%
Office Visit Copay
- Primary Care Physician $25 Copay
- Specialist Office Visit $60 Copay
- On-Line Visit $10 Copay
Out-of-Pocket Maximum (Calendar Yr)
- Individual $7,350
- Family $14,700
Hospitalization
- Inpatient Deductible, 30%
- Outpatient Deductible, 30%
Lab and X-Ray (non-complex) 30%
Lab and X-Ray (complex) Deductible, 30%
Emergency Services $250 Copay + 30%
Urgent Care $25 Copay
Preventive Care No Charge
Chiropractic/Acupuncture $25 Copay
Limited to 30 visits per year
Pharmacy Benefits
Pharmacy Deductible
- Individual (Except Tier 1) $250
Retail Pharmacy
- Tier 1 Generic Formulary $15 Copay
- Tier 2 Brand Name Formulary Deductible, $35 Copay
- Tier 3 Non-Formulary Deductible, 30% up to $350 per script
- Tier 4 Specialty Rx Deductible, 30% up to $350 per script
Retail Supply Limit 30 Days
Mail Order Pharmacy
- Tier 1 Generic Formulary $45 Copay
- Tier 2 Brand Name Formulary Deductible, $105 Copay
- Tier 3 Non-Formulary Deductible, 30% up to $350 per script
- Tier 4 Specialty Rx Deductible, 30% up to $350 per script
Mail Order Supply Limit 90 Days
6