
Page 11 - Catasys Benefit Guide 2020-2021
P. 11
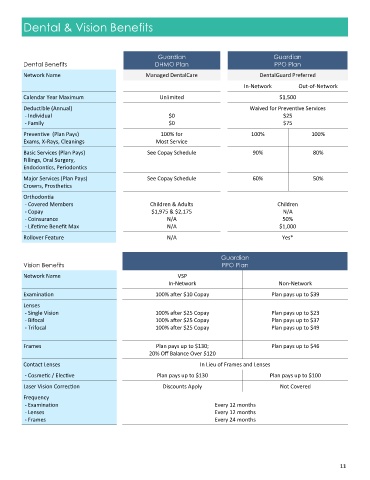
Dental & Vision Benefits
Guardian Guardian
Dental Benefits DHMO Plan PPO Plan
Network Name Managed DentalCare DentalGuard Preferred
In-Network Out-of-Network
Calendar Year Maximum Unlimited $1,500
Deductible (Annual) Waived for Preventive Services
- Individual $0 $25
- Family $0 $75
Preventive (Plan Pays) 100% for 100% 100%
Exams, X-Rays, Cleanings Most Service
Basic Services (Plan Pays) See Copay Schedule 90% 80%
Fillings, Oral Surgery,
Endodontics, Periodontics
Major Services (Plan Pays) See Copay Schedule 60% 50%
Crowns, Prosthetics
Orthodontia
- Covered Members Children & Adults Children
- Copay $1,975 & $2,175 N/A
- Coinsurance N/A 50%
- Lifetime Benefit Max N/A $1,000
Rollover Feature N/A Yes*
Guardian
Vision Benefits PPO Plan
Network Name VSP
In-Network Non-Network
Examination 100% after $10 Copay Plan pays up to $39
Lenses
- Single Vision 100% after $25 Copay Plan pays up to $23
- Bifocal 100% after $25 Copay Plan pays up to $37
- Trifocal 100% after $25 Copay Plan pays up to $49
Frames Plan pays up to $130; Plan pays up to $46
20% Off Balance Over $120
Contact Lenses In Lieu of Frames and Lenses
- Cosmetic / Elective Plan pays up to $130 Plan pays up to $100
Laser Vision Correction Discounts Apply Not Covered
Frequency
- Examination Every 12 months
- Lenses Every 12 months
- Frames Every 24 months
11