
Page 13 - Veritone EE California and Colorado Benefit Guide_2020
P. 13
PRESCRIPTION DRUG COVERAGE
Veritone’s medical plans include prescription drug coverage for you and your covered dependents.
Retail Pharmacy
Use a retail pharmacy to fill prescriptions for acute conditions (conditions that Pharmacy Tips
do not require the medication to be taken on a regular basis). At a Use generic and over the counter drugs when available. The best
participating pharmacy, you will receive up to a 30 day supply of your way to save on prescriptions is to use generic or over the counter
prescriptions. medications as opposed to brand name drugs. Generic drugs must use
the same active ingredients as the brand name version of the drug. A
Mail Order Pharmacy – Maintenance Medication generic drug must also meet the same quality and safety standards.
You could pay less for the same medication when you use the mail order
pharmacy. The mail order pharmacy is a fast, easy and convenient way to Use the mail order benefit for maintenance medications To save
save time and money on your maintenance medications (drugs that you need money and time, consider using the mail order pharmacy to fill your
to take regularly). You can order additional supplies of medication at a maintenance medications.
discount. See below for details!
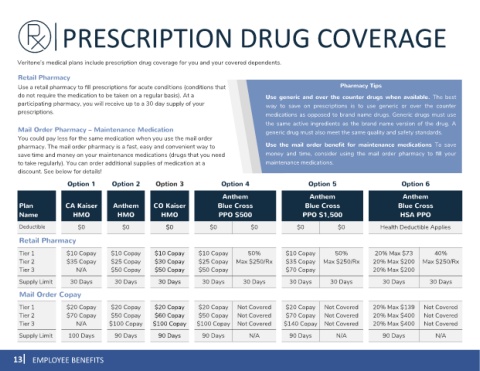
Option 1 1 Option 2 Option 3 Option 4 Option 5 Option 6
Anthem Anthem Anthem
Plan CA Kaiser Anthem CO Kaiser Blue Cross Blue Cross Blue Cross
Name HMO HMO HMO PPO $500 PPO $1,500 HSA PPO
Deductible $0 $0 $0 $0 $0 $0 $0 Health Deductible Applies
Retail Pharmacy
Tier 1 $10 Copay $10 Copay $10 Copay $10 Copay 50% $10 Copay 50% 20% Max $73 40%
Tier 2 $35 Copay $25 Copay $30 Copay $25 Copay Max $250/Rx $35 Copay Max $250/Rx 20% Max $200 Max $250/Rx
Tier 3 N/A $50 Copay $50 Copay $50 Copay $70 Copay 20% Max $200
Supply Limit 30 Days 30 Days 30 Days 30 Days 30 Days 30 Days 30 Days 30 Days 30 Days
Mail Order Copay
Tier 1 $20 Copay $20 Copay $20 Copay $20 Copay Not Covered $20 Copay Not Covered 20% Max $139 Not Covered
Tier 2 $70 Copay $50 Copay $60 Copay $50 Copay Not Covered $70 Copay Not Covered 20% Max $400 Not Covered
Tier 3 N/A $100 Copay $100 Copay $100 Copay Not Covered $140 Copay Not Covered 20% Max $400 Not Covered
Supply Limit 100 Days 90 Days 90 Days 90 Days N/A 90 Days N/A 90 Days N/A
13 EMPLOYEE BENEFITS