
Page 6 - Razer Benefits Guide 1-18 No CA
P. 6
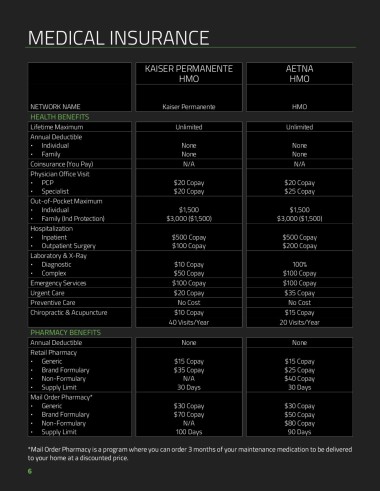
MEDICAL INSURANCE
KAISER PERMANENTE AETNA
HMO HMO
NETWORK NAME Kaiser Permanente HMO
HEALTH BENEFITS
Lifetime Maximum Unlimited Unlimited
Annual Deductible
• Individual None None
• Family None None
Coinsurance (You Pay) N/A N/A
Physician Office Visit
• PCP $20 Copay $20 Copay
• Specialist $20 Copay $25 Copay
Out-of-Pocket Maximum
• Individual $1,500 $1,500
• Family (Ind Protection) $3,000 ($1,500) $3,000 ($1,500)
Hospitalization
• Inpatient $500 Copay $500 Copay
• Outpatient Surgery $100 Copay $200 Copay
Laboratory & X-Ray
• Diagnostic $10 Copay 100%
• Complex $50 Copay $100 Copay
Emergency Services $100 Copay $100 Copay
Urgent Care $20 Copay $35 Copay
Preventive Care No Cost No Cost
Chiropractic & Acupuncture $10 Copay $15 Copay
40 Visits/Year 20 Visits/Year
PHARMACY BENEFITS
Annual Deductible None None
Retail Pharmacy
• Generic $15 Copay $15 Copay
• Brand Formulary $35 Copay $25 Copay
• Non-Formulary N/A $40 Copay
• Supply Limit 30 Days 30 Days
Mail Order Pharmacy*
• Generic $30 Copay $30 Copay
• Brand Formulary $70 Copay $50 Copay
• Non-Formulary N/A $80 Copay
• Supply Limit 100 Days 90 Days
*Mail Order Pharmacy is a program where you can order 3 months of your maintenance medication to be delivered
to your home at a discounted price.
6