
Page 5 - Marcus & Millichap Flipbook
P. 5
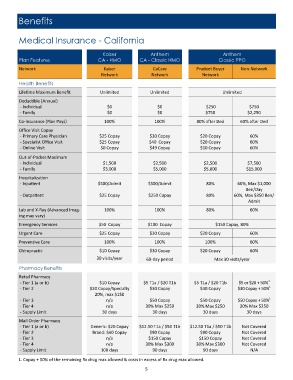
Benefits
Medical Insurance - California
Kaiser Anthem Anthem
Plan Features CA - HMO CA - Classic HMO Classic PPO
Network Kaiser CaCare z Prudent Buyer Non-Network
Network Network Network
Health Benefits
Lifetime Maximum Benefit Unlimited Unlimited Unlimited
Deductible (Annual)
- Individual $0 $0 $250 $750
- Family $0 $0 $750 $2,250
Co-Insurance (Plan Pays) 100% 100% 80% after Ded 60% after Ded
Office Visit Copay
- Primary Care Physician $25 Copay $30 Copay $20 Copay 60%
- Specialist Office Visit $25 Copay $40 Copay $20 Copay 60%
- Online Visit $0 Copay $49 Copay $10 Copay 60%
Out-of-Pocket Maximum
- Individual $1,500 $2,500 $2,500 $7,500
- Family $3,000 $5,000 $5,000 $15,000
Hospitalization
- Inpatient $500/Admit $500/Admit 80% 60%, Max $1,000
Ben/Day
- Outpatient $25 Copay $250 Copay 80% 60%, Max $350 Ben/
Admit
Lab and X-Ray (Advanced Imag‐ 100% 100% 80% 60%
ing may vary)
Emergency Services $50 Copay $100 Copay $150 Copay, 80%
Urgent Care $25 Copay $30 Copay $20 Copay 60%
Preventive Care 100% 100% 100% 60%
Chiropractic $10 Copay $30 Copay $20 Copay 60%
30 visits/year 60-day period Max 30 visits/year
Pharmacy Benefits
Retail Pharmacy
- Tier 1 (a or b) $10 Copay $5 T1a / $20 T1b $5 T1a / $20 T1b $5 or $20 + 50% 1
- Tier 2 $20 Copay/Specialty $30 Copay $30 Copay $30 Copay + 50% 1
20%, max $150
- Tier 3 n/a $50 Copay $50 Copay $50 Copay + 50% 1
- Tier 4 n/a 30% Max $250 30% Max $250 30% Max $250
- Supply Limit 30 days 30 days 30 days 30 days
Mail Order Pharmacy
- Tier 1 (a or b) Generic: $20 Copay $12.50 T1a / $50 T1b $12.50 T1a / $50 T1b Not Covered
- Tier 2 Brand: $40 Copay $90 Copay $90 Copay Not Covered
- Tier 3 n/a $150 Copay $150 Copay Not Covered
- Tier 4 n/a 30% Max $300 30% Max $300 Not Covered
- Supply Limit 100 days 90 days 90 days N/A
1. Copay + 50% of the remaining Rx drug max allowed & costs in excess of Rx drug max allowed.
5