
Page 10 - Work Life and Benefits Booklet 2018 - SS
P. 10
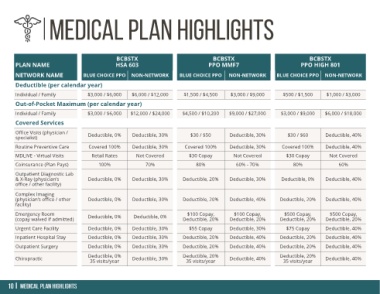
BCBSTX BCBSTX BCBSTX
PLAN NAME HSA 603 PPO MMF7 PPO HIGH 801
NETWORK NAME BLUE CHOICE PPO NON-NETWORK BLUE CHOICE PPO NON-NETWORK BLUE CHOICE PPO NON-NETWORK
Deductible (per calendar year)
Individual / Family $3,000 / $6,000 $6,000 / $12,000 $1,500 / $4,500 $3,000 / $9,000 $500 / $1,500 $1,000 / $3,000
Out-of-Pocket Maximum (per calendar year)
Individual / Family $3,000 / $6,000 $12,000 / $24,000 $4,500 / $10,200 $9,000 / $27,000 $3,000 / $9,000 $6,000 / $18,000
Covered Services
Office Visits (physician /
specialist) Deductible, 0% Deductible, 30% $30 / $50 Deductible, 30% $30 / $60 Deductible, 40%
Routine Preventive Care Covered 100% Deductible, 30% Covered 100% Deductible, 30% Covered 100% Deductible, 40%
MDLIVE - Virtual Visits Retail Rates Not Covered $30 Copay Not Covered $30 Copay Not Covered
Coinsurance (Plan Pays) 100% 70% 80% 60% - 70% 80% 60%
Outpatient Diagnostic Lab
& X-Ray (physician’s Deductible, 0% Deductible, 30% Deductible, 20% Deductible, 30% Deductible, 0% Deductible, 40%
office / other facility)
Complex Imaging
(physician’s office / other Deductible, 0% Deductible, 30% Deductible, 20% Deductible, 40% Deductible, 20% Deductible, 40%
facility)
Emergency Room $100 Copay, $100 Copay, $500 Copay, $500 Copay,
(copay waived if admitted) Deductible, 0% Deductible, 0% Deductible, 20% Deductible, 20% Deductible, 20% Deductible, 20%
Urgent Care Facility Deductible, 0% Deductible, 30% $55 Copay Deductible, 30% $75 Copay Deductible, 40%
Inpatient Hospital Stay Deductible, 0% Deductible, 30% Deductible, 20% Deductible, 40% Deductible, 20% Deductible, 40%
Outpatient Surgery Deductible, 0% Deductible, 30% Deductible, 20% Deductible, 40% Deductible, 20% Deductible, 40%
Deductible, 0% Deductible, 20% Deductible, 20%
Chiropractic 35 visits/year Deductible, 30% 35 visits/year Deductible, 40% 35 visits/year Deductible, 40%