
Page 10 - TCM EE Guide 2019 v2 FINAL
P. 10
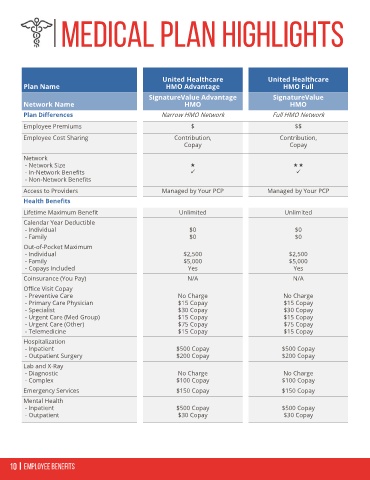
Medical Plan highlights
United Healthcare United Healthcare
Plan Name HMO Advantage HMO Full
SignatureValue Advantage SignatureValue
Network Name HMO HMO
Plan Differences Narrow HMO Network Full HMO Network
Employee Premiums $ $$
Employee Cost Sharing Contribution, Contribution,
Copay Copay
Network
- Network Size
- In-Network Benefits
- Non-Network Benefits
Access to Providers Managed by Your PCP Managed by Your PCP
Health Benefits
Lifetime Maximum Benefit Unlimited Unlimited
Calendar Year Deductible
- Individual $0 $0
- Family $0 $0
Out-of-Pocket Maximum
- Individual $2,500 $2,500
- Family $5,000 $5,000
- Copays Included Yes Yes
Coinsurance (You Pay) N/A N/A
Office Visit Copay
- Preventive Care No Charge No Charge
- Primary Care Physician $15 Copay $15 Copay
- Specialist $30 Copay $30 Copay
- Urgent Care (Med Group) $15 Copay $15 Copay
- Urgent Care (Other) $75 Copay $75 Copay
- Telemedicine $15 Copay $15 Copay
Hospitalization
- Inpatient $500 Copay $500 Copay
- Outpatient Surgery $200 Copay $200 Copay
Lab and X-Ray
- Diagnostic No Charge No Charge
- Complex $100 Copay $100 Copay
Emergency Services $150 Copay $150 Copay
Mental Health
- Inpatient $500 Copay $500 Copay
- Outpatient $30 Copay $30 Copay
10 Employee Benefits