
Page 14 - Volcom Benefit Summary 2019 National 2
P. 14
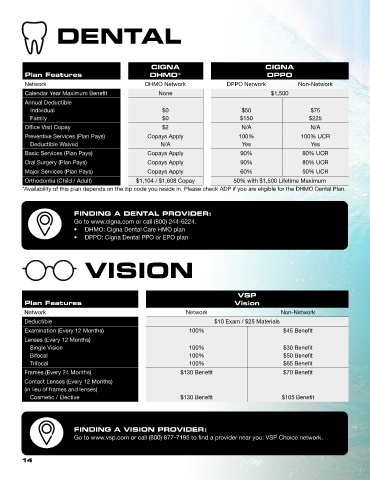
DENTAL
CIGNA CIGNA
Plan Features DHMO* DPPO
Network DHMO Network DPPO Network Non-Network
Calendar Year Maximum Benefit None $1,500
Annual Deductible
Individual $0 $50 $75
Family $0 $150 $225
Office Visit Copay $2 N/A N/A
Preventive Services (Plan Pays) Copays Apply 100% 100% UCR
Deductible Waived N/A Yes Yes
Basic Services (Plan Pays) Copays Apply 90% 80% UCR
Oral Surgery (Plan Pays) Copays Apply 90% 80% UCR
Major Services (Plan Pays) Copays Apply 60% 50% UCR
Orthodontia (Child / Adult) $1,104 / $1,608 Copay 50% with $1,500 Lifetime Maximum
*Availability of this plan depends on the zip code you reside in. Please check ADP if you are eligible for the DHMO Dental Plan.
FINDING A DENTAL PROVIDER:
Go to www.cigna.com or call (800) 244-6224.
• DHMO: Cigna Dental Care HMO plan
• DPPO: Cigna Dental PPO or EPO plan
VISION
VSP
Plan Features Vision
Network Network Non-Network
Deductible $10 Exam / $25 Materials
Examination (Every 12 Months) 100% $45 Benefit
Lenses (Every 12 Months)
Single Vision 100% $30 Benefit
Bifocal 100% $50 Benefit
Trifocal 100% $65 Benefit
Frames (Every 24 Months) $130 Benefit $70 Benefit
Contact Lenses (Every 12 Months)
(in lieu of frames and lenses)
Cosmetic / Elective $130 Benefit $105 Benefit
FINDING A VISION PROVIDER:
Go to www.vsp.com or call (800) 877-7195 to find a provider near you: VSP Choice network.
14