
Page 11 - Work Life and Benefits Booklet 2020 SE
P. 11
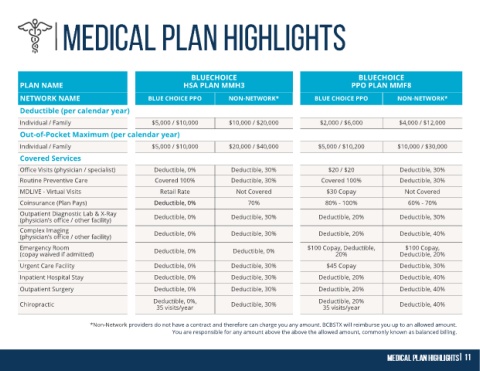
BLUECHOICE BLUECHOICE
PLAN NAME HSA PLAN MMH3 PPO PLAN MMF8
NETWORK NAME BLUE CHOICE PPO NON-NETWORK* BLUE CHOICE PPO NON-NETWORK*
Deductible (per calendar year)
Individual / Family $5,000 / $10,000 $10,000 / $20,000 $2,000 / $6,000 $4,000 / $12,000
Out-of-Pocket Maximum (per calendar year)
Individual / Family $5,000 / $10,000 $20,000 / $40,000 $5,000 / $10,200 $10,000 / $30,000
Covered Services
Office Visits (physician / specialist) Deductible, 0% Deductible, 30% $20 / $20 Deductible, 30%
Routine Preventive Care Covered 100% Deductible, 30% Covered 100% Deductible, 30%
MDLIVE - Virtual Visits Retail Rate Not Covered $30 Copay Not Covered
Coinsurance (Plan Pays) Deductible, 0% 70% 80% - 100% 60% - 70%
Outpatient Diagnostic Lab & X-Ray
(physician’s office / other facility) Deductible, 0% Deductible, 30% Deductible, 20% Deductible, 30%
Complex Imaging Deductible, 0% Deductible, 30% Deductible, 20% Deductible, 40%
(physician’s office / other facility)
Emergency Room $100 Copay, Deductible, $100 Copay,
(copay waived if admitted) Deductible, 0% Deductible, 0% 20% Deductible, 20%
Urgent Care Facility Deductible, 0% Deductible, 30% $45 Copay Deductible, 30%
Inpatient Hospital Stay Deductible, 0% Deductible, 30% Deductible, 20% Deductible, 40%
Outpatient Surgery Deductible, 0% Deductible, 30% Deductible, 20% Deductible, 40%
Deductible, 0%, Deductible, 20%
Chiropractic 35 visits/year Deductible, 30% 35 visits/year Deductible, 40%
*Non-Network providers do not have a contract and therefore can charge you any amount. BCBSTX will reimburse you up to an allowed amount.
You are responsible for any amount above the above the allowed amount, commonly known as balanced billing.