
Page 10 - Sea Dwelling EE Guide 01-20
P. 10
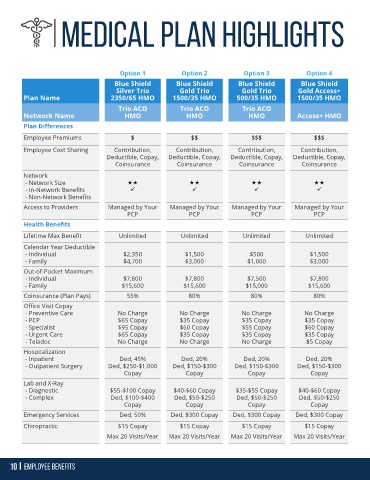
Option 1 Option 2 Option 3 Option 4
Blue Shield Blue Shield Blue Shield Blue Shield
Silver Trio Gold Trio Gold Trio Gold Access+
Plan Name 2350/65 HMO 1500/35 HMO 500/35 HMO 1500/35 HMO
Trio ACO Trio ACO Trio ACO
Network Name HMO HMO HMO Access+ HMO
Plan Differences
Employee Premiums $ $$ $$$ $$$
Employee Cost Sharing Contribution, Contribution, Contribution, Contribution,
Deductible, Copay, Deductible, Copay, Deductible, Copay, Deductible, Copay,
Coinsurance Coinsurance Coinsurance Coinsurance
Network
- Network Size
- In-Network Benefits ✓ ✓ ✓ ✓
- Non-Network Benefits
Access to Providers Managed by Your Managed by Your Managed by Your Managed by Your
PCP PCP PCP PCP
Health Benefits
Lifetime Max Benefit Unlimited Unlimited Unlimited Unlimited
Calendar Year Deductible
- Individual $2,350 $1,500 $500 $1,500
- Family $4,700 $3,000 $1,000 $3,000
Out-of-Pocket Maximum
- Individual $7,800 $7,800 $7,500 $7,800
- Family $15,600 $15,600 $15,000 $15,600
Coinsurance (Plan Pays) 55% 80% 80% 80%
Office Visit Copay
- Preventive Care No Charge No Charge No Charge No Charge
- PCP $65 Copay $35 Copay $35 Copay $35 Copay
- Specialist $95 Copay $60 Copay $55 Copay $60 Copay
- Urgent Care $65 Copay $35 Copay $35 Copay $35 Copay
- Teladoc No Charge No Charge No Charge $5 Copay
Hospitalization
- Inpatient Ded, 45% Ded, 20% Ded, 20% Ded, 20%
- Outpatient Surgery Ded, $250-$1,000 Ded, $150-$300 Ded, $150-$300 Ded, $150-$300
Copay Copay Copay Copay
Lab and X-Ray
- Diagnostic $55-$100 Copay $40-$60 Copay $35-$55 Copay $40-$60 Copay
- Complex Ded, $100-$400 Ded, $50-$250 Ded, $50-$250 Ded, $50-$250
Copay Copay Copay Copay
Emergency Services Ded, 50% Ded, $300 Copay Ded, $300 Copay Ded, $300 Copay
Chiropractic $15 Copay $15 Copay $15 Copay $15 Copay
Max 20 Visits/Year Max 20 Visits/Year Max 20 Visits/Year Max 20 Visits/Year