
Page 6 - Pathway EE Guide 06-17
P. 6
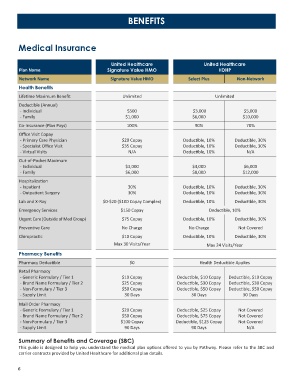
BENEFITS
Medical Insurance
United Healthcare United Healthcare
Plan Name Signature Value HMO HDHP
Network Name Signature Value HMO Select Plus Non-Network
Health Benefits
Lifetime Maximum Benefit Unlimited Unlimited
Deductible (Annual)
- Individual $500 $3,000 $5,000
- Family $1,000 $6,000 $10,000
Co-Insurance (Plan Pays) 100% 90% 70%
Office Visit Copay
- Primary Care Physician $20 Copay Deductible, 10% Deductible, 30%
- Specialist Office Visit $35 Copay Deductible, 10% Deductible, 30%
- Virtual Visits N/A Deductible, 10% N/A
Out-of-Pocket Maximum
- Individual $3,000 $4,000 $6,000
- Family $6,000 $8,000 $12,000
Hospitalization
- Inpatient 30% Deductible, 10% Deductible, 30%
- Outpatient Surgery 30% Deductible, 10% Deductible, 30%
Lab and X-Ray $0-$20 ($100 Copay Complex) Deductible, 10% Deductible, 30%
Emergency Services $150 Copay Deductible, 10%
Urgent Care (Outside of Med Group) $75 Copay Deductible, 10% Deductible, 30%
Preventive Care No Charge No Charge Not Covered
Chiropractic $10 Copay Deductible, 10% Deductible, 30%
Max 30 Visits/Year Max 24 Visits/Year
Pharmacy Benefits
Pharmacy Deductible $0 Health Deductible Applies
Retail Pharmacy
- Generic Formulary / Tier 1 $10 Copay Deductible, $10 Copay Deductible, $10 Copay
- Brand Name Formulary / Tier 2 $25 Copay Deductible, $30 Copay Deductible, $30 Copay
- Non-Formulary / Tier 3 $50 Copay Deductible, $50 Copay Deductible, $50 Copay
- Supply Limit 30 Days 30 Days 30 Days
Mail Order Pharmacy
- Generic Formulary / Tier 1 $20 Copay Deductible, $25 Copay Not Covered
- Brand Name Formulary / Tier 2 $50 Copay Deductible, $75 Copay Not Covered
- Non-Formulary / Tier 3 $100 Copay Deductible, $125 Copay Not Covered
- Supply Limit 90 Days 90 Days N/A
Summary of Benefits and Coverage (SBC)
This guide is designed to help you understand the medical plan options offered to you by Pathway. Please refer to the SBC and
carrier contracts provided by United Healthcare for additional plan details.
6