
Page 76 - New Hire Kit (Non-Union)
P. 76
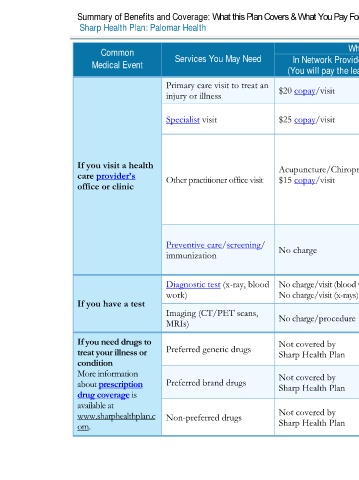
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2020 – 12/31/2020
Sharp Health Plan: Palomar Health Coverage for: Individual / Family | Plan Type: HMO
Common Services You May Need What You Will Pay Limitations, Exceptions, & Other
Medical Event In Network Provider Out-of-Network Provider Important Information
(You will pay the least) (You will pay the most)
Primary care visit to treat an
injury or illness $20 copay/visit Not covered None
Preauthorization is required, except for
Specialist visit $25 copay/visit Not covered
obstetric gynecologic services.
Acupuncture/Chiropractic coverage is
limited to 40 combined visits/calendar year
If you visit a health Acupuncture/Chiropractic: without preauthorization.
care provider’s Other practitioner office visit $15 copay/visit Not covered
office or clinic Cost sharing for covered supplemental
Acupuncture/Chiropractic services do not
count towards the out–of–pocket limit.
You may have to pay for services that
Preventive care/screening/ aren’t preventive. Ask your provider if
immunization No charge Not covered the services you need are preventive.
Then check what your plan will pay for.
Diagnostic test (x-ray, blood No charge/visit (blood work)
work) No charge/visit (x-rays) Not covered None
If you have a test
Imaging (CT/PET scans, No charge/procedure Not covered Preauthorization is required.
MRIs)
If you need drugs to Not covered by Not covered by
treat your illness or Preferred generic drugs Sharp Health Plan Sharp Health Plan
condition
More information Not covered by Not covered by Administered by CVS Caremark
about prescription Preferred brand drugs Sharp Health Plan Sharp Health Plan 800-776-1355 / Caremark.com
drug coverage is
available at
www.sharphealthplan.c Non-preferred drugs Not covered by Not covered by
om. Sharp Health Plan Sharp Health Plan
2 of 11
Palomar Health HMO NG 1 L / ACCH15_40 / VSA8