
Page 31 - 2021 Medical Plan SPD
P. 31
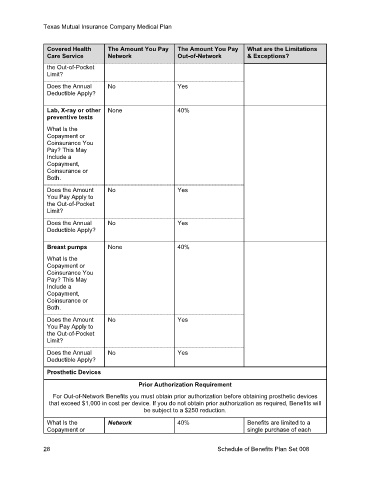
Texas Mutual Insurance Company Medical Plan
Covered Health The Amount You Pay The Amount You Pay What are the Limitations
Care Service Network Out-of-Network & Exceptions?
the Out-of-Pocket
Limit?
Does the Annual No Yes
Deductible Apply?
Lab, X-ray or other None 40%
preventive tests
What Is the
Copayment or
Coinsurance You
Pay? This May
Include a
Copayment,
Coinsurance or
Both.
Does the Amount No Yes
You Pay Apply to
the Out-of-Pocket
Limit?
Does the Annual No Yes
Deductible Apply?
Breast pumps None 40%
What Is the
Copayment or
Coinsurance You
Pay? This May
Include a
Copayment,
Coinsurance or
Both.
Does the Amount No Yes
You Pay Apply to
the Out-of-Pocket
Limit?
Does the Annual No Yes
Deductible Apply?
Prosthetic Devices
Prior Authorization Requirement
For Out-of-Network Benefits you must obtain prior authorization before obtaining prosthetic devices
that exceed $1,000 in cost per device. If you do not obtain prior authorization as required, Benefits will
be subject to a $250 reduction.
What Is the Network 40% Benefits are limited to a
Copayment or single purchase of each
28 Schedule of Benefits Plan Set 008